For years, I found myself unable to utter the phrase, “my ostomy bag saved my life.” It felt like a claim reserved for those with clear-cut, textbook diagnoses—patients with inflammatory bowel disease (IBD), acute diverticulitis, or stage-four colon cancer. These are conditions with measurable pathology, where the binary choice of “to bag or not to bag” is backed by clear clinical evidence. My path was different. My condition was invisible, poorly understood by the medical establishment, and deeply intertwined with a complex, systemic connective tissue disorder: Ehlers-Danlos Syndrome (EDS).
Today, on my two-year "stoma-versary," I am sharing my story not just as a patient, but as an advocate. If you are living with EDS and find yourself doubled over in pain, or if you are a medical provider struggling to treat a patient whose symptoms defy traditional diagnostic labels, this narrative is for you.
Understanding the Anatomy of an Ostomy
Before delving into the complexities of my journey, it is vital to define what an ostomy is. An ostomy is a surgical procedure that creates an opening, known as a stoma, in the abdominal wall. This allows waste to bypass the traditional route—the rectum—and exit the body into an external pouching system.
There are various types of ostomies, each serving different clinical needs:
- End Ileostomy: The small intestine is brought to the surface of the abdomen. In my case, this was a permanent procedure following the removal of my colon.
- Loop Ostomy: A loop of the bowel is brought to the surface, typically intended as a temporary diversion.
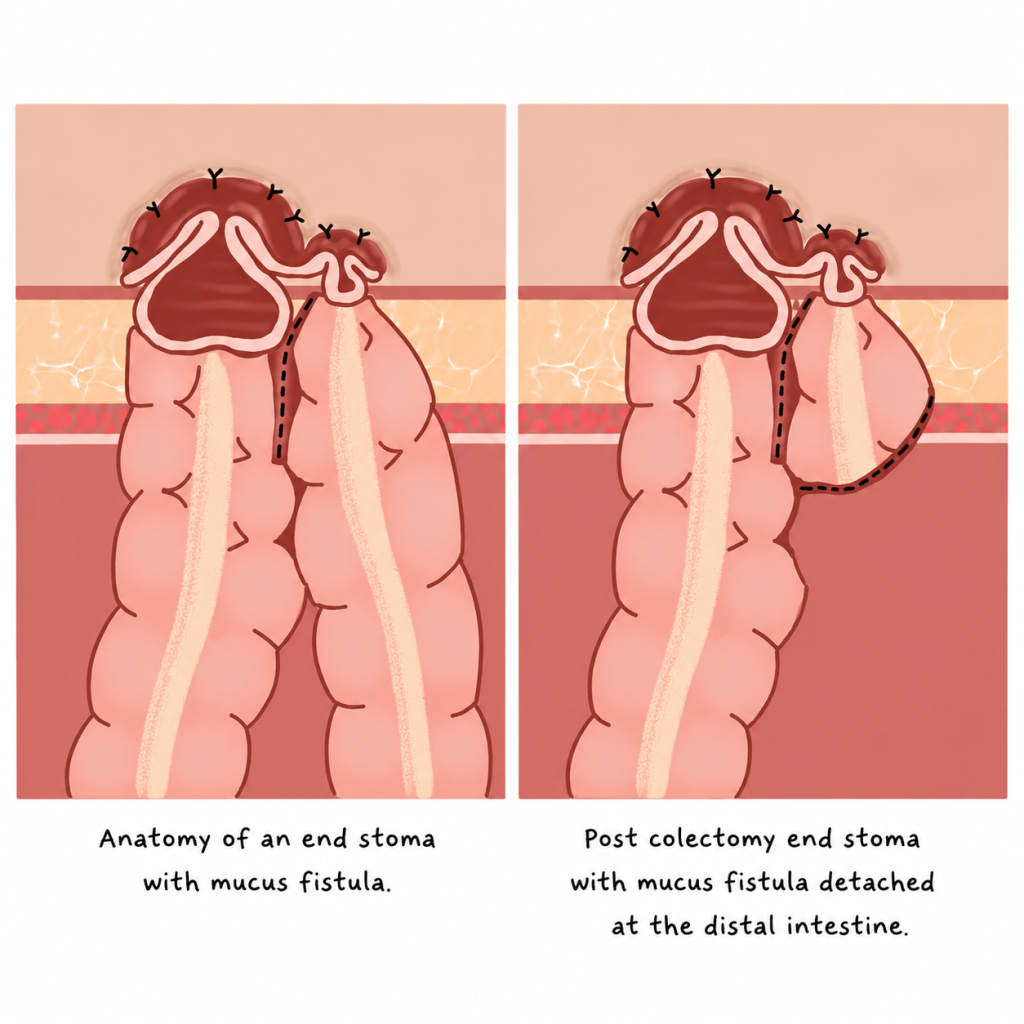
- End Stoma with Mucus Fistula: Used when the large intestine remains in the body, but the primary exit is diverted.
For me, the decision to undergo a permanent ileostomy was the culmination of a lifetime of struggle, not a sudden medical crisis.
The EDS Connection: When Scaffolding Fails
Ehlers-Danlos syndrome (EDS) is a group of hereditary connective tissue disorders. To understand EDS, think of connective tissue as the body’s internal scaffolding. It provides structure, strength, and elasticity to joints, skin, blood vessels, and organs. When this scaffolding is faulty, the entire system suffers.
While many associate EDS exclusively with joint hypermobility—the "bendy" nature of the disorder—it is profoundly multisystemic. For me, the most debilitating manifestation was in my gastrointestinal (GI) tract.
A Lifetime of "Just Constipation"
My medical history reads like a catalog of dismissed pain. I cannot recall a time before the stomach aches. As a child, I spent elementary school hallways doubled over in agony. By middle school, I was a fixture in the bathroom, trapped in a cycle of physiological failure. By high school, I had learned to weaponize humor to hide the reality of my condition, masking deep-seated embarrassment with jokes about my digestive woes.

By college, my symptoms had shifted from merely embarrassing to truly debilitating. I became a prisoner in my own home, trapped by a body that refused to function. I underwent a gamut of recommended treatments: aggressive laxatives, specialized diets, physical therapy, and endless consultations with gastroenterologists. None of it worked. My symptoms included:
- Chronic, severe abdominal distention.
- Total bowel motility failure.
- Intractable, multi-day cycles of pain.
- The profound psychological toll of living with a body that felt fundamentally broken.
The Diagnostic Cascade: Bridging the Gap
The road to a diagnosis was not a straight line; it was a labyrinth. When a specialist finally moved beyond standard testing, we began to uncover the reality: my GI issues were not idiopathic. They were the result of structural failures linked to my EDS.
The diagnostic journey involved a series of intensive, often overlooked tests:
- Defecography: To assess the structural integrity of the pelvic floor and rectal evacuation.
- Sitz Marker Studies: To measure the speed of transit through the colon.
- Manometry: To evaluate the muscle function of the GI tract.
- Advanced Imaging: To look for visceroptosis—a condition where organs "drop" or shift due to weakened connective tissues.
Throughout this process, I found myself in the position of teacher, often providing my own research to radiologists to ensure they knew what to look for. The diagnosis revealed that my organs were literally failing to hold their place, leading to a mechanical obstruction that no amount of diet or medication could fix.
The Choice: Facing the Permanent
When my colorectal surgeon suggested a permanent ostomy, the word "permanent" caused a visceral, physical reaction. The anxieties were overwhelming: Will it leak? Will I smell? Will people still find me attractive? Will my contamination OCD spiral?
I spent months grappling with these fears. However, I eventually realized I was suffering from self-gaslighting. I was treating my current, miserable existence as a baseline, when in reality, it was a state of chronic, unnecessary suffering. The prospect of an ostomy wasn’t a loss of normalcy; it was an opportunity to reclaim a life that had been stolen by pain.
Surgery and the Road to Recovery
My surgical journey was two-fold. First, the creation of the stoma brought immediate, life-altering relief. The constant bloating and heaviness that had defined my life for decades vanished. A year later, I underwent a total colectomy—a ten-hour procedure to remove over seven feet of non-functioning colon.
The recovery was not linear. As any EDS patient knows, healing is rarely textbook. I faced complications and had to advocate for myself from the hospital bed, but the trade-off was clear: the moment the ostomy was functional, I was no longer dying; I was living.
Implications: Building a New Life
Since my recovery, I have pivoted from a patient to an advocate. I founded a small business creating custom ostomy bag covers, transforming a medical necessity into a form of self-expression. My advocacy has taken me across the globe, including a trip to Kenya with Campaign 52 to provide resources to women in need.
Living with an ostomy is not without its challenges. Leaks occur. Skin irritation is real. There is a grieving process for the life you thought you’d have. But there is also a community. The isolation I once felt—being one of the few with a diagnosis like visceroptosis—has been replaced by a digital network of survivors and thrivers.
Key Takeaways for Patients and Providers
To my fellow EDS patients: You are not imagining your pain. "Just constipation" is a dismissive term for a potentially life-altering condition. If your symptoms are treatment-resistant, keep searching for a provider who understands the link between connective tissue and GI dysfunction.
To medical providers: When a patient with EDS presents with a lifelong history of GI dysfunction, please look beyond standard motility drugs. Investigate the structural, the "rare," and the mechanical. Your patients are not exaggerating; they are often the most knowledgeable experts on their own suffering.
Two years ago, I feared that an ostomy would end my life as I knew it. Today, I know with absolute certainty that it was the only way to begin the life I was meant to lead. My ostomy didn’t take my dignity; it gave me the freedom to exist without pain.
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, visceroptosis, or ostomies. Discussion of diagnostic testing, surgical interventions, and treatment outcomes is provided for educational purposes only and should not be interpreted as medical advice. Readers should consult their healthcare team regarding their individual circumstances.