




Introduction: Two Disasters, One Pattern of Negligence
In April 2010, the world watched in horror as the Deepwater Horizon oil rig exploded in the Gulf of Mexico. It was a catastrophe of unprecedented proportions: eleven lives were lost instantly, and for 87 days, an estimated 210 million gallons of raw crude oil gushed into the ocean. The environmental fallout was staggering, contaminating over 1,000 miles of coastline and decimating marine ecosystems for a generation. The cause was eventually traced to a "perfect storm" of corporate negligence, faulty equipment, and a systemic disregard for safety protocols in favor of profit.
However, a growing chorus of medical researchers and advocates argues that a second, even more pervasive "man-made disaster" is unfolding away from the cameras. They contend that the field of modern psychiatry, through over-prescription and the systematic "soiling" of patients with potent chemical compounds, has created a public health crisis that rivals the greatest environmental disasters in history. Just as the BP oil spill was the result of ignored warnings and institutional failures, critics suggest that the "psychiatric spill" is the result of a medical-industrial complex that prioritizes pharmaceutical compliance over patient recovery.
Main Facts: The Scale of the "Psychiatric Spill"
The comparison between an oil spill and psychiatric care is not merely metaphorical; it is based on the scale of human and economic loss. While the BP disaster resulted in $69 billion in fines and settlements, the human cost of what some call "biological psychiatry" is measured in mortality rates.
According to research based on placebo-controlled randomized trials and long-term cohort studies, psychiatric medications are now estimated to be the third leading cause of death in Western societies, trailing only heart disease and cancer. This mortality is attributed to a range of factors, including the metabolic effects of antipsychotics, the increased risk of falls and fractures in the elderly, and the paradoxical increase in suicidal ideation associated with certain antidepressants.
Furthermore, the "contamination" of the patient population is vast. Hundreds of millions of individuals globally are currently prescribed one or more psychiatric drugs. Data suggests that approximately 50% of long-term antidepressant users experience significant difficulty when attempting to discontinue their medication. These individuals suffer from withdrawal symptoms—often mislabeled by clinicians as a "relapse" of the original condition—that range from severe anxiety and insomnia to physical "brain zaps" and cognitive impairment.
Chronology: From Chemical Imbalance to Systemic Dependency
To understand how psychiatry reached this point, one must trace the evolution of the "chemical imbalance" narrative.
The Rise of the Biological Model (1980s–1990s)
In the late 20th century, psychiatry underwent a paradigm shift. Moving away from psychodynamic and social models of distress, the field embraced a purely biological approach. This era saw the introduction of Selective Serotonin Reuptake Inhibitors (SSRIs) like Prozac. Marketing campaigns convinced both doctors and the public that mental distress was the result of a "chemical imbalance" in the brain—a theory that has since been largely debunked by neuroscientific research but remains a potent cultural myth.
The Era of Polypharmacy (2000s–Present)
As the "chemical imbalance" theory took root, the prescribing of multiple drugs (polypharmacy) became the norm rather than the exception. Patients who did not respond to an initial antidepressant were often "augmented" with antipsychotics or mood stabilizers. This created a generation of patients "soiled" in a cocktail of chemicals, much like the wildlife caught in the 2010 Gulf spill.
The Discovery of the Withdrawal Crisis
By the mid-2010s, the "spill" became impossible to ignore. Online communities of patients began documenting the harrowing process of trying to quit these drugs. It became clear that the clinical guidelines for withdrawal—which often suggested a fast taper over two to four weeks—were not only inadequate but dangerous. The medical establishment’s slow response to this data mirrors BP’s initial attempts to downplay the volume of oil leaking from the Macondo well.
Supporting Data: The Economics and Ethics of Harm
The data supporting the "disaster" narrative in psychiatry is multifaceted, involving clinical, economic, and ethical dimensions.
Mortality and Disability
Research highlights that the widespread use of psychiatric drugs has not led to a decrease in the prevalence of mental illness or disability. On the contrary, in many developed nations, the number of people on disability pensions for mental health reasons has risen in tandem with the increase in prescriptions. Critics point to the long-term "toxic" effects of drugs like Lithium and Clozapine, which require constant monitoring of kidney and liver function, as evidence of the high price patients pay for symptom management.

The Failure of Tapering Guidelines
Until very recently, official medical guidelines suggested "halving the dose" at each step of a taper. However, pharmacological data shows that the relationship between drug dose and brain receptor occupancy is not linear but hyperbolic. This means that the most significant changes in the brain occur at the lowest doses. A 50% reduction from a small dose is much more impactful than a 50% reduction from a high dose. By failing to recognize this, psychiatrists have inadvertently trapped millions of patients in a cycle of dependency, misinterpreting withdrawal-induced distress as a return of the "disease."
Accountability and Fines
While BP was held legally and financially accountable for its negligence, the pharmaceutical industry and psychiatric leadership have largely avoided similar repercussions. Despite numerous lawsuits regarding the suppressed data of drug harms, the industry continues to exert a "superpower" influence over medical education, research funding, and government policy.
Official Responses: Institutional Inertia vs. Global Calls for Reform
The response from the psychiatric establishment has been mixed, often characterized by a defensive posture that protects the status quo.
The Resistance of "Biological Psychiatry"
Leading psychiatric organizations have been slow to acknowledge the scale of the drug-withdrawal crisis. Many prominent psychiatrists continue to defend the biological model, citing the benefits of medication for acute crises while downplaying the risks of long-term use. This "organized denial" is a central theme for critics who argue that the profession is more interested in its own prestige and its relationship with the pharmaceutical industry than in objective patient outcomes.
The Global Pivot: UN and WHO
In a surprising turn, international bodies have begun to side with the critics. The United Nations and the World Health Organization (WHO) have issued reports calling for a "revolution" in mental health. These reports emphasize that the over-medicalization of human distress is a violation of human rights and that social determinants—such as poverty, trauma, and inequality—are more significant drivers of mental health issues than chemical imbalances. They have called for a shift toward "person-centered" care that prioritizes social support and the safe reduction of medication.
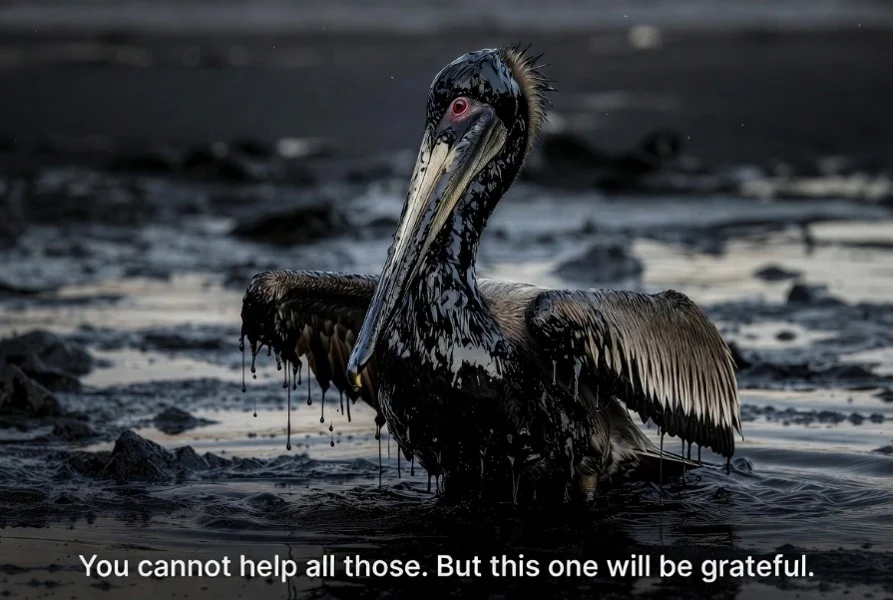
Implications: The "Pelican Philosophy" and the Path Forward
The story of the Deepwater Horizon includes a poignant anecdote of a rescuer cleaning a single oil-soaked pelican. When told that his efforts made no difference because thousands more were dying, the rescuer replied: "It makes a difference to this one." This "Pelican Philosophy" is now the guiding light for a growing movement of "deprescribing" specialists.
The Individual Rescue
Individual case studies highlight the life-changing impact of proper withdrawal support. One patient in Europe, who had been on a cocktail of Lithium and Clozapine for 30 years due to family dysfunction rather than a clear biological illness, found himself abandoned by his local doctors when he asked for help tapering. It was only through independent networks—such as the Critical Psychiatry Network and the International Institute for Psychiatric Drug Withdrawal—that he was able to find specialists like Maria Kelly and Eve Keighley. These practitioners utilize "hyperbolic tapering," reducing doses by tiny increments over months or years, allowing the brain to heal.
The Need for Infrastructure
To address the "spill" at a systemic level, advocates argue for the creation of:
- 24-Hour National Helplines: Dedicated to drug withdrawal and crisis support.
- Drug Withdrawal Centers: Facilities that provide free, non-medicalized support for those transitioning off psychiatric medication.
- Educational Reform: Re-training nurses, social workers, and teachers to help citizens avoid psychiatric labels and drugs rather than acting as "compliance officers."
Conclusion: Holding the Rig Owners Accountable
The BP oil spill eventually stopped because the well was capped and the company was forced to pay for the cleanup. In psychiatry, the "well" of over-prescription is still gushing. For the "disaster" to end, there must be a fundamental shift in accountability.
The movement for reform is not just about safer tapering; it is about reclaiming the human experience from a narrow, medicalized framework. As the "psychiatric spill" continues to affect millions, the goal remains clear: to help the "oil-soaked" patients fly again, one by one, while fighting for a world where such a man-made catastrophe is no longer possible. The hope is that, like the environmental movement before it, the movement for psychiatric reform will eventually "overcome" the institutional inertia of the current system.