








In a professional landscape increasingly defined by polarized views on psychopharmacology, a significant intellectual skirmish has erupted between the psychiatric establishment and its internal critics. The catalyst for this latest exchange is a rebuttal authored by Bryan Shapiro, MD, published on his Substack, targeting a recent high-profile article in the Psychiatric Times.
The original piece, titled “The Top 10 Misleading Claims About Antidepressants,” was penned by two of the field’s most prominent figures: Roger McIntyre, MD, and Ronald Pies, MD. In their article, McIntyre and Pies sought to debunk what they characterize as common misconceptions that undermine public confidence in Selective Serotonin Reuptake Inhibitors (SSRIs) and other antidepressants. However, Dr. Shapiro’s response—shared via the critical psychiatry platform Mad in America—argues that it is the establishment’s defense, rather than the criticism, that lacks scientific rigor.
Shapiro’s rebuttal represents more than just a difference of opinion; it is a "rapid-fire, scientific rebuttal" that claims the Psychiatric Times article contains misleading assertions not substantiated by fundamental pharmacological principles. As the debate over the efficacy, safety, and biological mechanisms of antidepressants intensifies, the rift within the medical community suggests a looming paradigm shift in how mental health is understood and treated.
Main Facts: A Collision of Perspectives
At the heart of the dispute is the "chemical imbalance" theory of depression and the interpretation of clinical trial data. For decades, the public was told that depression was caused by a lack of serotonin, which antidepressants corrected. While many modern psychiatrists have distanced themselves from this simplistic model, the legacy of the theory remains a point of contention.
The Core Arguments of McIntyre and Pies
In the Psychiatric Times, McIntyre and Pies argued that critics of antidepressants often rely on "straw man" arguments. They contended that:
- Antidepressants are effective beyond a placebo effect.
- The "chemical imbalance" theory was never the primary scientific explanation used by the profession (a claim critics find revisionist).
- The risks of withdrawal and long-term side effects are often exaggerated by "anti-psychiatry" activists.
The Shapiro Counter-Argument
Dr. Bryan Shapiro’s rebuttal systematically deconstructs these claims. He asserts that the Psychiatric Times authors have overlooked the "fundamental pharmacological principles" that govern how these drugs interact with the human brain. Shapiro focuses on the "hyperbolic" nature of receptor binding—where the majority of a drug’s effect occurs at very low doses—and argues that clinical trials often fail to account for the complexities of drug withdrawal, which can be mistaken for a relapse of the original condition.
Notably, Shapiro’s rebuttal excludes items five and six of the original list—which concern suicidal and homicidal associations with antidepressants—focusing instead on the biological and clinical data regarding efficacy and physiological dependence.
Chronology: The Evolution of a Medical Controversy
To understand the weight of this exchange, one must look at the timeline of antidepressant discourse over the last two decades.
2004–2008: The First Wave of Skepticism
The controversy began to gain mainstream traction when researchers like Irving Kirsch used Freedom of Information Act (FOIA) requests to access unpublished FDA data. Kirsch’s findings suggested that for the majority of patients with mild to moderate depression, the difference between an antidepressant and a placebo was "clinically insignificant."
2022: The Moncrieff Umbrella Review
A major turning point occurred in July 2022, when Dr. Joanna Moncrieff and her colleagues published a massive "umbrella review" in Molecular Psychiatry. The study concluded there was no consistent evidence of a link between serotonin levels and depression. This sparked a global media firestorm, forcing the psychiatric establishment to defend the utility of SSRIs despite the lack of a clear biological mechanism.
2023–2024: The Establishment Strikes Back
In response to the growing "critical psychiatry" movement, major publications like the Psychiatric Times began publishing defenses of the status quo. The McIntyre and Pies article was intended to be a definitive "fact-check" to silence critics.
July 2024: The Shapiro Rebuttal
Dr. Shapiro’s response marks the latest entry in this timeline. By moving the debate from the pages of traditional medical journals to Substack and Mad in America, Shapiro exemplifies a new era of "guerrilla peer review," where independent clinicians use digital platforms to challenge institutional narratives in real-time.
Supporting Data: The Science of the Rebuttal
Dr. Shapiro’s critique is grounded in several technical areas of psychopharmacology that he argues are frequently ignored by proponents of widespread antidepressant use.
1. The Hamilton Depression Rating Scale (HAM-D) Discrepancy
A central piece of supporting data in this debate involves the HAM-D scale, the gold standard for measuring antidepressant efficacy. Shapiro points out that while antidepressants often show a "statistically significant" improvement over placebos, the actual difference on the 52-point HAM-D scale is often only about 1.8 to 2 points. Critics argue that such a small difference is imperceptible to the patient and the clinician, failing the threshold for "clinical significance" set by organizations like the National Institute for Health and Care Excellence (NICE).
2. Receptor Occupancy and Hyperbolic Curves
Shapiro brings attention to the "dose-response" curve of SSRIs. Pharmacological data shows that even at very low doses (e.g., 2mg of citalopram), a significant percentage of serotonin transporters are blocked. This "hyperbolic" curve explains why tapering off these medications is so difficult; the most profound changes in brain chemistry happen during the final milligrams of a dose reduction. Shapiro argues that McIntyre and Pies fail to acknowledge this, leading to a dismissal of the severity of withdrawal symptoms.
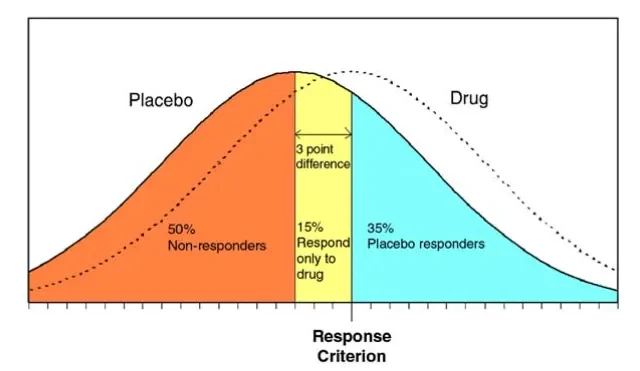
3. The "Unblinding" Effect
Another critical data point is the "active placebo" problem. Because antidepressants cause side effects (like dry mouth or nausea), patients in clinical trials often realize they are not in the placebo group. This "unblinding" can lead to an enhanced placebo effect, where the patient’s expectation of improvement—rather than the drug’s chemical action—drives the results. Shapiro suggests that when trials are properly blinded, the "drug effect" often vanishes.
Official Responses and the Institutional Stance
The response from the broader psychiatric community has been split along ideological lines.
The Institutional View
The American Psychiatric Association (APA) and many leading academic departments continue to support the use of antidepressants as a first-line treatment. Their official stance is that while the exact mechanism of depression is complex (the "biopsychosocial model"), the empirical evidence from decades of clinical practice shows that these drugs help millions of people. Figures like McIntyre and Pies represent this institutional view, emphasizing that the risks of untreated depression—including disability and death—far outweigh the risks of the medication.
The Critical Response
Organizations like Mad in America provide a platform for what they call "science, psychiatry, and social justice." Their response to the Psychiatric Times article has been one of deep skepticism. They view the original article as an attempt to "gaslight" patients who have suffered from long-term side effects or difficult withdrawal.
In his Substack, Shapiro notes that the Psychiatric Times article relies on "low-quality evidence" and ignores the lived experience of patients. This sentiment is echoed by many in the "lived experience" community, who feel that the medical establishment is more interested in protecting its professional reputation than in investigating the potential harms of its treatments.
Implications: The Future of Mental Health Care
The debate between Shapiro and the Psychiatric Times authors has profound implications for the future of clinical practice and patient safety.
Informed Consent
One of the most significant implications is the need for a total overhaul of the informed consent process. If the "chemical imbalance" theory is indeed a myth, and if the efficacy of the drugs is marginal for many, patients must be told this before starting a regimen. Shapiro’s critique suggests that current informed consent is often based on outdated or misleading information.
The Tapering Crisis
As the understanding of "hyperbolic" receptor binding becomes more mainstream, there is an urgent need for "deprescribing" protocols. Many patients find themselves "trapped" on antidepressants not because their depression has returned, but because the withdrawal symptoms are so severe they cannot quit. This has led to the rise of specialized tapering clinics and the use of compounded liquid medications to allow for the minute dose reductions Shapiro advocates for.
A Shift Toward Holistic Models
The ongoing struggle to prove the biological superiority of antidepressants is pushing some in the field toward a "social" or "psychological" model of distress. If the "brain fix" is not as effective as once thought, psychiatry may be forced to return to its roots in psychotherapy, lifestyle intervention, and addressing social determinants of health such as poverty, isolation, and trauma.
Conclusion: A Field in Transition
The exchange between Dr. Bryan Shapiro and Drs. McIntyre and Pies is not merely an academic exercise. It is a battle for the soul of psychiatry. On one side is a traditional model that views mental distress through a medical lens, prioritizing pharmacological intervention. On the other is a growing movement of "whistleblower" clinicians and researchers who demand a more transparent, evidence-based, and cautious approach.
As Dr. Shapiro’s rebuttal continues to circulate through the medical community, it serves as a reminder that science is never "settled." The "rapid-fire" critique of the Psychiatric Times may well be a harbinger of a new era in which the fundamental pillars of modern psychiatry are rebuilt on a foundation of greater pharmacological honesty and patient-centered care.