










In the high-stakes world of clinical psychiatry, a burgeoning intellectual conflict has moved from the pages of medical journals to the digital public square. The latest flashpoint involves a "rapid-fire" scientific rebuttal by Dr. Bryan Shapiro, a psychiatrist who has taken aim at a recent article published in the Psychiatric Times. The original piece, authored by two of the field’s most prominent figures—Dr. Roger McIntyre and Dr. Ronald Pies—titled “The Top 10 Misleading Claims About Antidepressants,” sought to debunk common criticisms of Selective Serotonin Reuptake Inhibitors (SSRIs) and related medications.
However, Dr. Shapiro’s response, published via his Substack, suggests that the "debunking" effort itself may be built on a foundation of "misleading claims" and "inadequate quality evidence." This exchange highlights a deepening schism in psychiatry regarding the efficacy, safety, and biological mechanisms of the most commonly prescribed medications in the Western world.
Main Facts: A Clash of Perspectives
The crux of the dispute centers on how antidepressants are represented to both the medical community and the general public. On one side, Drs. McIntyre and Pies represent the institutional "standard of care." Their article in Psychiatric Times was designed to provide clinicians with talking points to counter what they perceive as misinformation—specifically, the idea that antidepressants are no better than placebos, that they are "addictive," or that they are based on a "mythical" chemical imbalance.
Dr. Shapiro’s rebuttal, however, asserts that the institutional narrative is frequently out of step with fundamental pharmacological principles. He argues that by dismissing critical viewpoints as "misleading," the institutional guard is actually obscuring the complexities and potential harms of these drugs.
The debate touches on several key domains:
- The Serotonin Hypothesis: Whether the "chemical imbalance" theory was a legitimate scientific hypothesis or a marketing tool.
- Efficacy vs. Clinical Significance: The gap between a "statistically significant" improvement on a depression scale and a meaningful change in a patient’s life.
- Withdrawal vs. Discontinuation: The terminology used to describe the physiological distress experienced when stopping antidepressants.
- The Nature of Evidence: What constitutes "high-quality" evidence in a field heavily influenced by industry-funded trials.
Notably, Dr. Shapiro’s rebuttal explicitly excludes items 5 and 6 of the original article, which deal with the controversial associations between antidepressants and suicidal or homicidal ideation, focusing instead on the pharmacological and clinical efficacy claims.
Chronology: The Evolution of the Controversy
To understand the weight of this current exchange, one must look at the timeline of the "antidepressant wars" over the last two decades.
- The Late 1980s – 1990s: The "Prozac Era" begins. SSRIs are marketed heavily under the "chemical imbalance" theory, suggesting that depression is caused by a lack of serotonin in the synaptic cleft. This period sees a massive surge in prescriptions.
- 2008: Dr. Irving Kirsch and colleagues publish a meta-analysis in PLOS Medicine using Freedom of Information Act (FOIA) data from the FDA. They conclude that the difference between antidepressants and placebos is clinically negligible for most patients, except those with the most severe depression.
- 2011 – 2019: The rise of the "Critical Psychiatry" movement. Organizations like Mad in America begin providing a platform for doctors and patients to discuss long-term side effects and the difficulty of tapering off medications.
- July 2022: Dr. Joanna Moncrieff and colleagues publish an "umbrella review" in Molecular Psychiatry, concluding there is no consistent evidence of a link between low serotonin and depression. This creates a media firestorm.
- Late 2023: In response to the growing skepticism, Drs. McIntyre and Pies publish their "Top 10" list in Psychiatric Times, aiming to stabilize the narrative and reassure clinicians.
- Early 2024: Dr. Bryan Shapiro releases his point-by-point rebuttal, marking a new phase where younger, digitally-active clinicians are directly challenging the "Old Guard" of academic psychiatry.
Supporting Data: Examining the Pharmacological Rebuttal
Dr. Shapiro’s critique is rooted in what he describes as "fundamental pharmacological principles." One of the primary points of contention involves the "Chemical Imbalance" narrative.
The Serotonin Question
While Drs. Pies and McIntyre have argued that psychiatry "never really believed" in a simple chemical imbalance, Shapiro points to decades of pharmaceutical marketing and clinical practice where this was the primary explanation given to patients. He argues that if the serotonin theory is as weak as recent reviews suggest, then the mechanism of action for SSRIs remains largely unknown, making the "misleading" label for critics unfair.
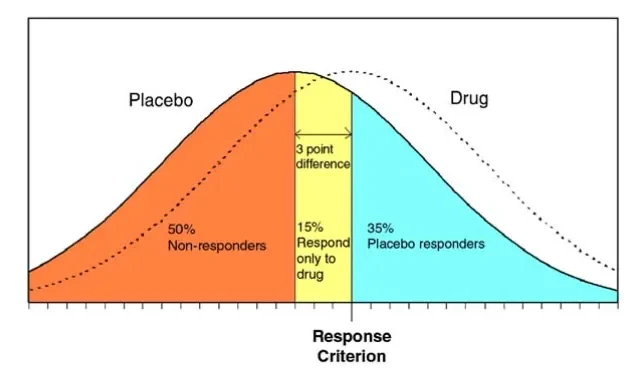
The Placebo Gap and the HAM-D Scale
A significant portion of the debate rests on the Hamilton Depression Rating Scale (HAM-D). Institutional defenders often point to the fact that SSRIs consistently outperform placebos in clinical trials. Shapiro, however, aligns with critics who note that the difference—often only 2 or 3 points on a 52-point scale—is "statistically significant" but not "clinically significant."
Supporting data for Shapiro’s view includes:
- The 3-Point Rule: The National Institute for Health and Care Excellence (NICE) in the UK previously suggested that a 3-point difference on the HAM-D is the minimum for clinical relevance. Many antidepressant trials fail to meet this threshold.
- Blinding Issues: Shapiro notes that side effects (like dry mouth or nausea) often "unblind" patients in trials, leading them to realize they are on the active drug, which enhances the placebo effect.
Withdrawal vs. "Discontinuation Syndrome"
Shapiro’s rebuttal takes a hard line on the term "discontinuation syndrome." He argues this is a euphemism created by the pharmaceutical industry to avoid the stigma of "withdrawal." Data from surveys of long-term users suggest that withdrawal symptoms can be severe, lasting months or even years—a reality that Shapiro claims is minimized in the Psychiatric Times article.
Official Responses: The Institutional Stance
While Dr. Shapiro’s rebuttal has gained traction among reform-minded medical professionals, the institutional response remains firm. Dr. Ronald Pies has long maintained that psychiatry employs a "biopsychosocial model," and that the "chemical imbalance" was always a "useful metaphor" rather than a literal biological fact.
In the original Psychiatric Times piece, McIntyre and Pies emphasize:
- Clinical Utility: They argue that regardless of the exact biological mechanism, millions of patients report improved quality of life on these medications.
- Safety Profiles: They contend that modern antidepressants are significantly safer than the older Tricyclic antidepressants (TCAs) and Monoamine Oxidase Inhibitors (MAOIs).
- The Danger of "Misinformation": They suggest that overly critical views of antidepressants may scare patients away from life-saving treatment, leading to increased rates of untreated depression and suicide.
However, Shapiro counters this by stating that "misleading" patients about the efficacy and difficulty of stopping these drugs is a violation of Informed Consent. He argues that the medical community cannot claim to be following "evidence-based medicine" if it selectively ignores data regarding the modest benefits and significant risks of long-term use.
Implications: The Future of Mental Health Care
The conflict between Dr. Shapiro and the authors of the Psychiatric Times article is more than a professional spat; it represents a paradigm shift in how society views mental health.
1. The Crisis of Informed Consent
If Shapiro’s critiques are valid, it suggests that many patients are not being fully informed about the nature of the drugs they are prescribed. The implication is that "Informed Consent" must include a discussion about the small "placebo-vs-drug" gap and the potential for long-term withdrawal.
2. The Move Toward Hyperbolic Tapering
As the debate over withdrawal intensifies, more clinicians are moving away from the "standard" two-week taper. Inspired by critics like Shapiro and the research of Dr. Mark Horowitz, there is a growing movement toward "hyperbolic tapering"—reducing doses by tiny increments over months or years to allow the brain to adjust.
3. The Search for New Models
The dismantling of the serotonin hypothesis (or at least its simplification) is forcing psychiatry to look for new models. Whether it is neuroplasticity, gut-brain axis research, or social-determinant models, the field is in a state of flux.
4. The Role of Independent Media
The fact that this debate is occurring on platforms like Substack and Mad in America highlights the declining influence of traditional medical journals, which many perceive as being too close to the pharmaceutical industry. "Rapid-fire rebuttals" from independent clinicians are becoming a primary source of information for a new generation of skeptical patients and doctors.
Conclusion
The rebuttal by Dr. Bryan Shapiro serves as a potent reminder that in the realm of medicine, "consensus" is often a moving target. By challenging the Psychiatric Times, Shapiro is not necessarily arguing that antidepressants should never be used, but rather that the scientific community must be more honest about what they do, what they don’t do, and what we simply do not yet know. As this debate continues to unfold, the ultimate winners should be the patients, who deserve a mental health system built on transparency, rigorous science, and a deep respect for the complexities of human biology.







