










For years, the experience was consistent: a Friday evening dinner plan, a familiar restaurant, and a mental block as impenetrable as a brick wall. "You know the place," the speaker would plead with her partner, gesturing vaguely as if to summon the name of a local establishment from thin air. "The one with the peanut shells on the floor… by the vet?" Hours later, the word—Texas Roadhouse—would finally surface, unbidden and far too late.
This isn’t merely the forgetfulness associated with aging. For many women in their late 40s and early 50s, this "sludginess" is a defining feature of a deeper, more pervasive phenomenon: menopause-related brain fog. What begins as a missing proper noun often metastasizes into an inability to focus during the workday, a profound sense of mental haziness, and an emotional volatility that feels entirely alien.
The Chronology of a Misdiagnosis
The journey for many women facing these symptoms is often marked by a frustrating odyssey through the medical system. The common narrative follows a predictable, yet disheartening, trajectory:
- The Initial Decline: In the late 40s, mental clarity begins to wane. The "morning burst" of productivity shrinks from eight hours to a mere two or three.
- The Medical Revolving Door: Patients seek help, often describing feelings of despair, lethargy, and cognitive depletion.
- The Conventional Misstep: Lacking specialized training in menopausal health, practitioners frequently pivot to antidepressants or sleep aids. For many, these treatments fail to address the root cause, sometimes exacerbating the sensation of feeling "zombified" or drugged.
- The Discovery: It is often only during a routine gynecological checkup—when symptoms like vaginal dryness or sleep disturbances are mentioned—that the true culprit is revealed.
- The Resolution: Upon the introduction of hormone therapy (estradiol and progesterone), the "switch" is flipped. Clarity returns, sleep stabilizes, and the fog lifts.
Supporting Data: Why "Brain Fog" Is Not Just in Your Head
Menopause is not a disease; it is a life stage. Yet, the physiological transition carries significant weight. According to the American College of Obstetricians and Gynecologists, approximately 40 percent of women report increased irritability, anxiety, and difficulty concentrating during the menopausal transition.
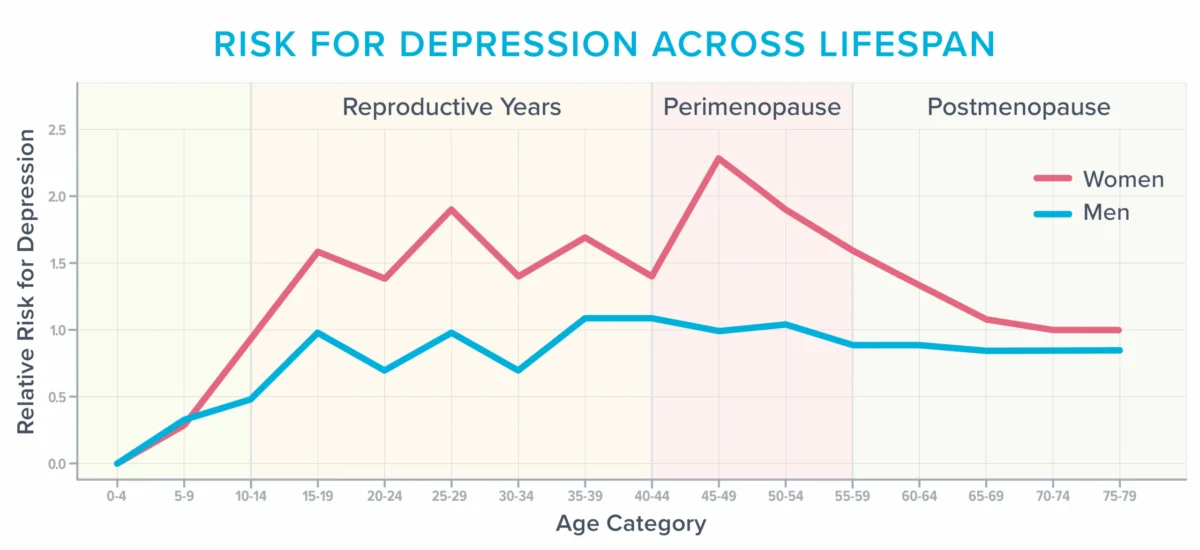
Crucially, the data suggests that women’s risk of depression peaks significantly during the perimenopausal years. This is not merely a psychological reaction to life stressors; it is a biological vulnerability.
The Vasomotor Connection
For years, hot flashes and night sweats were dismissed as minor inconveniences. Research now suggests they are markers of systemic physiological change. During a hot flash, norepinephrine and cortisol levels spike, blood vessels dilate, and heart rates accelerate.
Recent neuroimaging studies have provided alarming evidence: women who experience frequent hot flashes often exhibit an abundance of "white matter hyperintensities" in the brain. These lesions, once dismissed as signs of standard aging, are now recognized as predictors of future cognitive decline, doubling the risk of dementia and tripling the risk of future stroke in affected populations.
Official Responses and the "Defensive Medicine" Barrier
The medical community is currently grappling with a significant knowledge gap. Surveys indicate that 80 percent of medical residents feel "barely comfortable" discussing menopause, and few residency programs provide formal training on the subject.
This lack of expertise leads to what Dr. Jerrold H. Weinberg, a menopause-trained gynecologist, calls "defensive medicine." Clinicians, fearful of litigation based on decades-old, misinterpreted studies regarding hormone replacement therapy (HRT) and breast cancer risk, often shy away from providing effective treatment.
However, current consensus among experts—including those at the Menopause Society—is clear: for women under the age of 60 who are within 10 years of menopause onset, the benefits of hormone therapy often far outweigh the risks. Beyond alleviating cognitive and emotional distress, MHT may offer protective benefits against osteoporosis and Alzheimer’s disease.

The Intersection of Sleep and Cognition
The "insomnia" reported by many menopausal women is frequently a symptom of nocturnal hot flashes, even when the patient does not wake up drenched in sweat. The surge in cortisol that accompanies a vasomotor event causes frequent, micro-arousals.
These interruptions prevent the brain from performing essential "housekeeping," such as clearing metabolic toxins and consolidating memories. This sleep deprivation triggers the amygdala—the brain’s emotional center—to become hyper-reactive. The result is a cycle of irritability, anxiety, and reduced capacity for learning. When healthcare providers use the PHQ-9 depression scale, these menopausal symptoms are often misidentified as clinical depression, leading to the prescription of inappropriate medication.
Strategies for Advocacy and Recovery
Navigating this life stage requires a proactive, evidence-based approach.
1. Advocate for Specialized Care
Seek practitioners certified by the Menopause Society. When meeting with a physician, bring documented data. Avoid vague complaints; use specific metrics, such as: "I wake up five times a night, with a maximum of three hours of continuous sleep."
2. Implement Lifestyle Fundamentals
While there is no "magic diet" for menopause, the fundamentals of health—nutrition, physical activity, and stress management—are non-negotiable.
- Creatine Supplementation: Research suggests 5 to 7 grams of creatine monohydrate daily may help reduce mental fatigue and support mood.
- Light Exposure: Morning sunlight is essential for regulating the circadian rhythm and improving sleep quality.
- Exercise Modification: Middle age requires a shift in fitness. While vigorous movement is beneficial, high-intensity sessions should be balanced with recovery to avoid overtaxing the nervous system.
- Cognitive Behavioral Therapy for Insomnia (CBT-I): This is a gold-standard, non-pharmacological approach to restoring healthy sleep patterns.
3. Re-evaluating Responsibilities
Perhaps the most profound implication of the menopausal transition is the necessity of "downsizing" one’s mental load. Many women in their 40s and 50s are at the peak of their professional and personal responsibilities. This stage acts as an existential mirror, forcing a critical question: Do I need to be doing this?
Implications: The Hidden Opportunity
The transition through menopause, while physically and mentally taxing, offers a rare, forced opportunity for self-reflection. By shedding unnecessary commitments and prioritizing recovery, many women find that they emerge not just back to their "old selves," but into a more intentional version of their lives.
The "fog" is not a permanent state; it is a signal. By recognizing the biological underpinnings of these symptoms, advocating for appropriate hormone therapy when needed, and adopting lifestyle strategies that support brain health, women can navigate this transition with clarity. As the narrative of menopause continues to shift from a taboo subject to a recognized medical priority, the goal is clear: to ensure that the middle years are defined by wisdom and energy, rather than a struggle for mental survival.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional regarding hormonal therapies or changes to your medical regimen.








