







For many, the phrase "my ostomy bag saved my life" is synonymous with a battle against inflammatory bowel disease (IBD), acute diverticulitis, or the stark reality of colon cancer. These conditions carry clear, quantifiable pathology—visible evidence that dictates the medical necessity of surgical intervention. However, for those living with Ehlers-Danlos syndrome (EDS), the journey to such a life-altering procedure is often far more ambiguous, fraught with years of medical gaslighting, diagnostic dead ends, and invisible, systemic suffering.
As I mark my two-year "stoma-versary," I am sharing my story not just as a patient, but as an advocate. If you are navigating the complex intersection of EDS and gastrointestinal (GI) dysfunction, or if you are a medical provider struggling to treat "treatment-resistant" patients, it is time to look beyond the obvious.
Understanding the Ostomy: A Clinical Necessity
Before delving into the complexities of EDS-related GI failure, it is essential to define the procedure. An ostomy is a surgical intervention that creates an opening, or stoma, in the abdominal wall. This allows waste to bypass the rectum and exit the body into an external collection pouch.
There are several variations of this procedure:
- End Ileostomy: The small intestine is brought to the surface, and the colon is often bypassed or removed. This is the procedure I underwent to address chronic dysmotility.
- Loop Ostomy: A loop of the bowel is brought to the surface, often used for temporary diversions to allow distal sections of the bowel to heal.
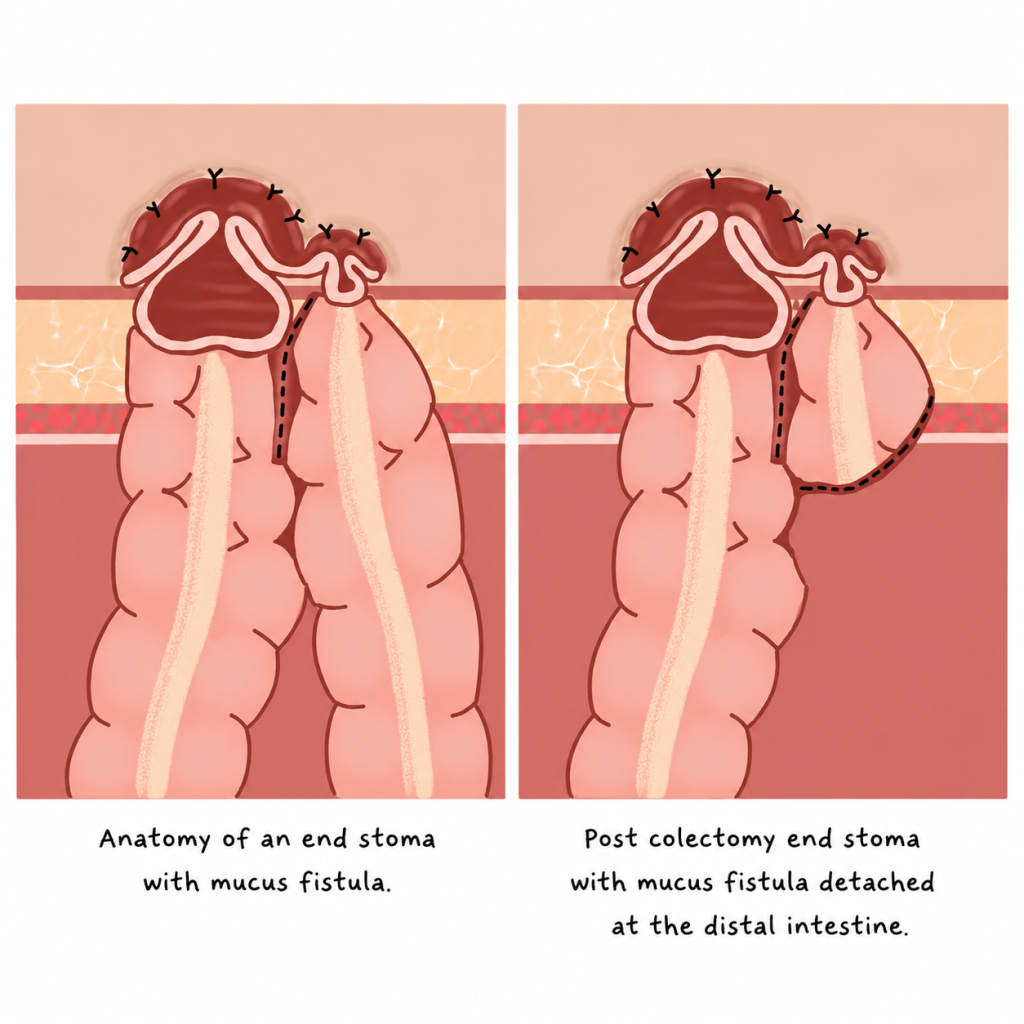
- End Stoma with Mucus Fistula: A complex configuration where the large intestine remains in the body while an end stoma is created, a method often employed in cases of extreme structural compromise.
The EDS Connection: When Scaffolding Fails
Ehlers-Danlos syndrome is a group of connective tissue disorders that affects the body’s "scaffolding." Because connective tissue provides the structural integrity for our skin, joints, blood vessels, and internal organs, EDS is inherently multisystemic.
While the public perception of EDS is often limited to "bendy joints," the reality for many patients involves profound autonomic and structural dysfunction in the gastrointestinal tract. In my case, my EDS manifested as severe, treatment-resistant GI failure.
A Lifetime of "Just Constipation": A Chronology of Decline
My struggle did not begin in adulthood; it was the backdrop of my entire life. From elementary school hallways, where I was doubled over in pain, to the middle school bathrooms where I sat for hours in silence, my childhood was defined by a malfunctioning gut.

By college, what was once "embarrassing" had become "debilitating." I was homebound, paralyzed by a combination of physical agony and the psychological toll of chronic illness. Despite adhering to every medical recommendation—from aggressive laxative regimens and specialized diets to pelvic floor physical therapy—my condition worsened. At my lowest point, I faced:
- Chronic, severe abdominal distention that made breathing difficult.
- Total dependence on bowel stimulants that eventually ceased to function.
- A psychological spiral caused by the persistent, unaddressed nature of my pain.
The Diagnostic Cascade: Bridging the Gap
The road to a diagnosis was a grueling, multi-year odyssey. When I finally found a GI specialist who viewed my history through the lens of connective tissue pathology, we began a targeted diagnostic cascade.
Unlike the common path, my diagnostic journey required me to act as the primary coordinator between radiologists and surgeons. I had to advocate for specialized imaging, including transit studies and dynamic evaluations, to prove that my bowels were not merely "lazy," but structurally compromised. These tests ultimately revealed significant visceroptosis—a condition where the organs descend below their normal position—coupled with profound dysmotility.
It was only when the visual evidence of these structural failures was presented that the medical community acknowledged what I had known for years: my body was not functioning because its support system had failed.
The Decision: Navigating Fear and Gaslighting
When my colorectal surgeon suggested a permanent ostomy, the term "permanent" triggered a wave of existential anxiety. I was haunted by the same questions that plague every patient facing this surgery:
- Will the bag leak?
- How will this impact my intimacy and social life?
- Will my existing OCD regarding contamination be exacerbated?
- What if this, too, fails?
Looking back, the most dangerous hurdle was not the surgery itself, but the self-gaslighting. I had been told for so long that my symptoms were "not that bad" or "manageable" that I struggled to trust my own desire for relief. I had to learn that choosing a radical medical intervention to reclaim my quality of life was not a failure—it was a survival strategy.
Surgery and Recovery: The Reality of Healing
My path to wellness was not a straight line. I first underwent a stoma creation, which provided immediate, life-changing relief from the pressure and pain. A year later, I underwent a total colectomy, removing over seven feet of non-functional colon.
The recovery was arduous. For anyone with EDS, healing is rarely textbook. My tissues did not respond to sutures with the expected consistency, and I had to remain a fierce advocate for my own care while recovering in a hospital bed. Yet, the outcome was undeniable: the moment my ostomy was functional, the decades-long weight of chronic bloating and dysfunction evaporated.
Implications for Patients and Providers
The impact of this journey has extended far beyond my own physical recovery. Living with an ostomy inspired me to launch a small business sewing custom bag covers, a creative outlet that transformed into a platform for community building. My work now includes international advocacy, including providing education and resources in Kenya for women with pelvic and colorectal disorders.
Key Takeaways for the Community:
- Trust Your Intuition: If you are an EDS patient with chronic GI symptoms, your experience is valid. "Just constipation" is a dismissive term for what may be a serious, systemic failure.
- Advocate for Specialized Imaging: Standard tests may not capture the structural nuances of EDS. Don’t hesitate to ask for, or seek, second opinions from specialists familiar with connective tissue disorders.
- Grief is Part of the Process: It is okay to be scared of the surgery, and it is okay to grieve the body you had before. These emotions do not invalidate the necessity of the procedure.
A Message to Medical Providers:
When a patient presents with a lifetime of treatment-resistant GI dysfunction, do not default to labeling it as psychosomatic or "mild." Investigate the structural, connective-tissue-based possibilities. Your willingness to look deeper can prevent years of unnecessary suffering and, in many cases, truly save a life.
Conclusion
My ostomy bag is not a symbol of illness; it is a tool of empowerment. It represents the end of a long, isolating silence and the beginning of a life reclaimed. For those standing on the precipice of this decision, I want you to know that there is a version of your life that is not only livable but vibrant, waiting for you on the other side.
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, visceroptosis, or ostomies. Discussion of diagnostic testing, surgical interventions, and treatment outcomes is provided for educational purposes only and should not be interpreted as medical advice. Readers should consult their healthcare team regarding their individual circumstances.