












As Ehlers-Danlos Syndrome (EDS) Awareness Month draws to a close, the medical and patient communities find themselves at a crossroads. While clinical understanding of connective tissue disorders has evolved, a cavernous gap remains between medical literature and the lived experience of patients. To bridge this divide, we spotlight four individuals—Jeevan Mann, Kaleena Deshawn, Krista Brack, and Jacqueline Teti—whose lives challenge the prevailing misconceptions surrounding EDS and Hypermobility Spectrum Disorder (HSD).
By examining their journeys, we aim to dismantle harmful stereotypes, illuminate the staggering "invisible" labor required to survive these conditions, and foster a culture of empathy for those navigating the complexities of chronic illness.

The Core Reality: Dispelling Prevalent Myths
The myths surrounding EDS and HSD are not merely annoying; they are dangerous barriers to timely diagnosis and effective treatment. These misconceptions—ranging from the gender-essentialist view that men do not "get" the condition to the dangerous "invisible illness" bias—serve to isolate patients and alienate them from the care they desperately need.
Myth 1: “Men Can’t Have EDS”
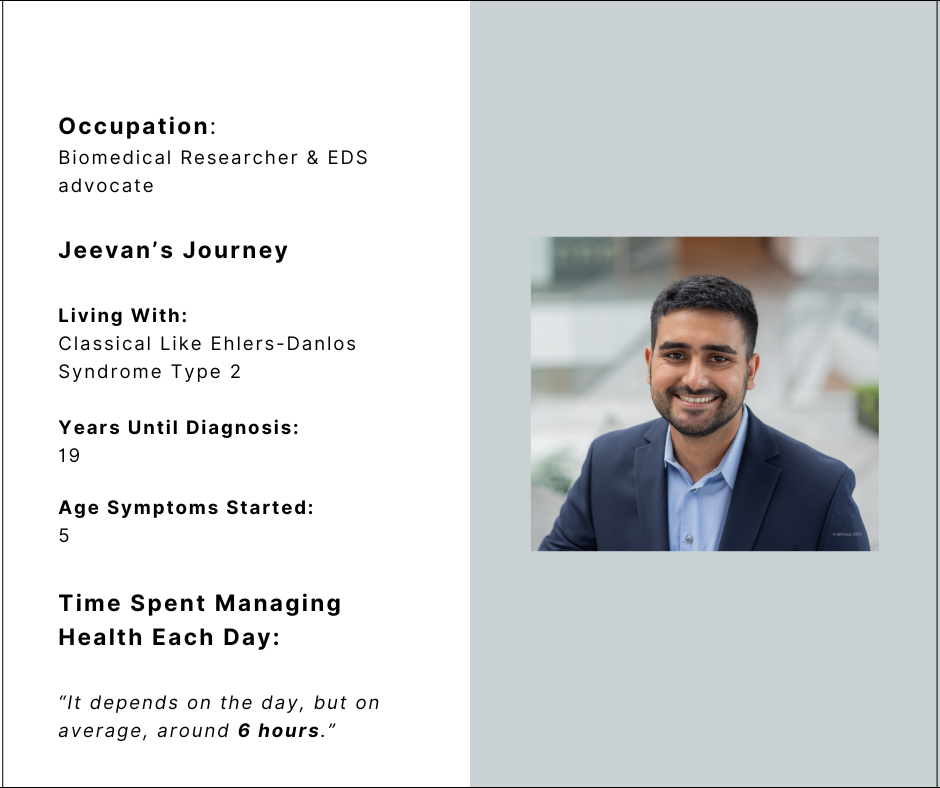
The stereotype that EDS is a condition exclusive to women is a persistent, medically inaccurate narrative. Jeevan Mann, a biomedical researcher and EDS advocate, serves as a powerful counter-narrative. Despite being diagnosed with Classical-Like Ehlers-Danlos Syndrome Type 2, his path to recognition took 19 years. His experience highlights a systemic failure to look for connective tissue disorders in male patients, often delaying critical interventions.
Myth 2: “EDS Doesn’t Affect People from All Backgrounds”
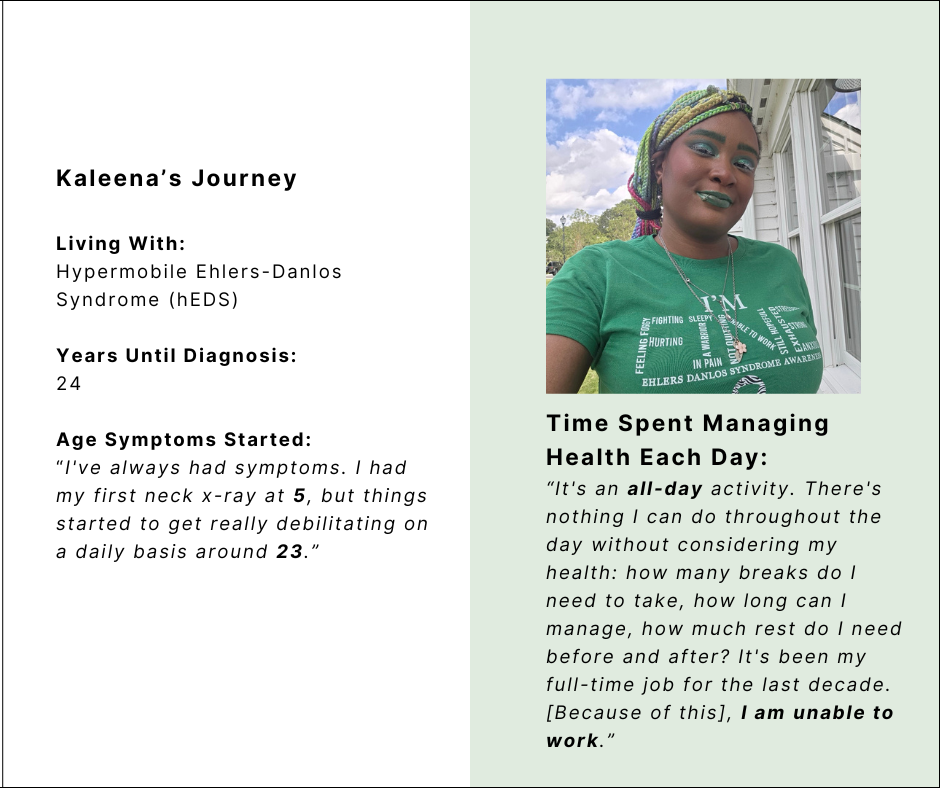
The notion that EDS is a "European disease" is a significant hurdle for patients of color. Kaleena Deshawn, who lives with Hypermobile EDS (hEDS), found that many support spaces were predominantly white, reinforcing the exclusionary myth that Black individuals were not prone to these genetic disorders. This lack of intersectional representation in support groups can leave patients feeling isolated and invalidated by the very communities meant to offer solace.
Myth 3: “EDS is Just Being a Bit ‘Bendy’”
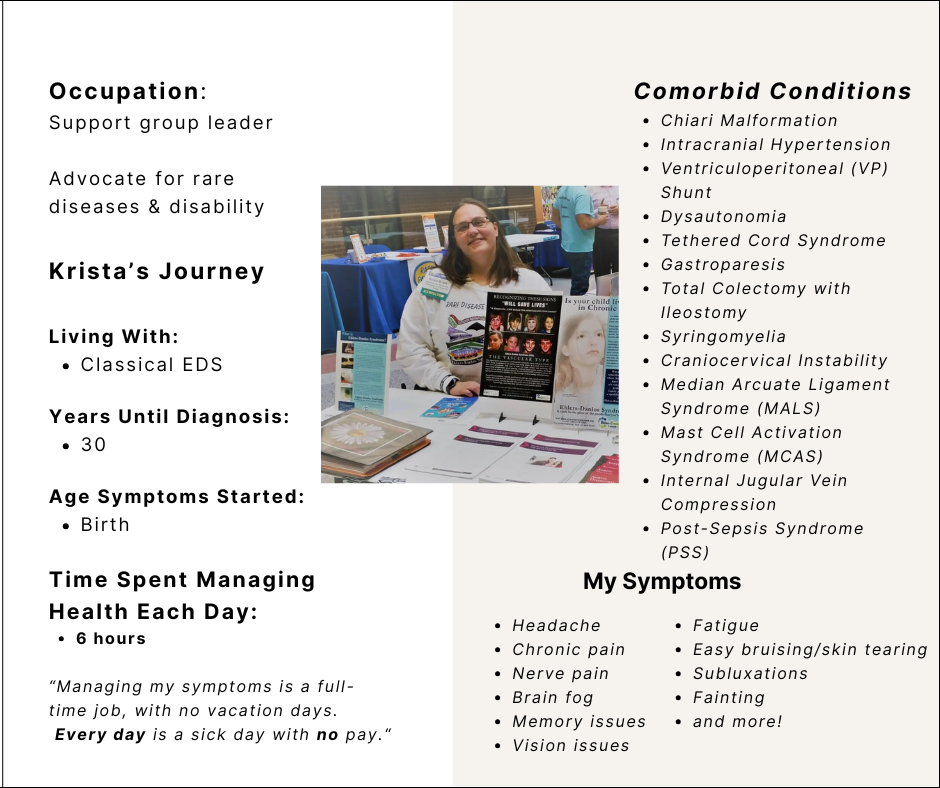
The colloquial dismissal of EDS as "hyper-mobility" or being "bendy" minimizes the systemic, multi-organ impact of the disease. Krista Brack, a support group leader living with Classical EDS, illustrates that the condition is far from a harmless flexibility. For Krista, managing her condition—which includes comorbidities like Chiari Malformation, Gastroparesis, and Internal Jugular Vein Compression—is a full-time, unpaid job.
Myth 4: “If You Were Actually Sick, You Would Look Sick”
The "invisible" nature of these conditions often invites judgment from medical professionals and the public alike. Jacqueline Teti, an editor and program director living with HSD, emphasizes that the external appearance of "wellness" hides a grueling internal reality. The pressure to "pass" as healthy leads to the invalidation of pain, forcing patients to constantly justify their medical needs.
Chronology of the Patient Experience
The road to an EDS/HSD diagnosis is rarely linear. It is a marathon marked by medical gaslighting, diagnostic delays, and the slow accumulation of comorbid conditions.
- Early Childhood: Many patients exhibit symptoms from birth or early childhood. Krista Brack reports symptoms since birth, while Jeevan Mann began showing signs at age 5.
- The "Gap" Years: On average, our featured individuals waited between 19 and 30 years for a formal diagnosis. These years are characterized by a "diagnostic odyssey," where patients are frequently dismissed, misdiagnosed, or told their symptoms are psychosomatic.
- The Turning Point: The transition from "undiagnosed" to "diagnosed" rarely brings immediate relief. Instead, it marks the beginning of a lifetime of intensive management.
- The Present Reality: For all four individuals, the daily routine is dominated by symptom management. Whether it is Jeevan Mann’s six-hour daily commitment or Jacqueline Teti’s three-to-four-hour regimen of physical therapy and medical coordination, the labor of living with EDS is constant.
Supporting Data: The "Invisible" Workload
To quantify the reality of life with EDS/HSD, we must look at the time, energy, and resources consumed by these conditions.
The Time Tax
Living with EDS is a full-time occupation. Our participants report spending, on average, between 3 and 6 hours per day on active symptom management. This includes:
- Physical therapy and specialized exercises to prevent subluxations.
- Coordination of complex medical appointments across multiple specialties.
- Management of comorbidities, such as Mast Cell Activation Syndrome (MCAS), POTS, and gastrointestinal issues.
- Navigating the "energy envelope"—the delicate, often impossible task of rationing limited energy for basic tasks like bathing, eating, or working.
The Comorbidity Load
EDS/HSD rarely travels alone. The systemic nature of connective tissue issues often leads to a cascade of secondary conditions. Among our four participants, we see a recurring pattern of:
- Dysautonomia/POTS: Affecting heart rate and blood pressure regulation.
- Neurological Involvement: Including Chiari Malformation, Craniocervical Instability, and intracranial hypertension.
- Immune/Gastrointestinal Issues: MCAS and Celiac disease.
This "comorbidity load" turns a single diagnosis into a complex web of care, requiring patients to become amateur experts in several medical fields just to advocate for their own safety.
Official Responses and Medical Advocacy
The lack of specialized training among primary care physicians and emergency room staff is a recurring theme in the testimonies of our participants. Krista Brack reports that her life has been put at risk multiple times due to hospital staff failing to recognize the nuances of her EDS-related complications.
The Need for Systemic Change
The medical community is slowly beginning to respond. Organizations like Chronic Pain Partners and international research groups are pushing for:

- Mandatory EDS/HSD Education: Integrating connective tissue disorder training into medical school curricula to reduce the diagnostic gap.
- Multidisciplinary Care Models: Moving away from siloed specialist care toward clinics that treat the patient holistically, acknowledging that POTS, MCAS, and EDS are often inextricably linked.
- Emergency Protocols: Establishing clear, accessible medical protocols for EDS patients in ER settings to prevent life-threatening errors during acute crises.
Implications: Building a Future of Inclusion and Advocacy
The stories of Jeevan, Kaleena, Krista, and Jacqueline are not just accounts of suffering; they are stories of profound resilience and ambition.
The Power of Representation
As Kaleena Deshawn notes, the exclusion of marginalized voices in support groups is a form of secondary trauma. Advocacy must be intersectional. For the EDS community to grow, it must actively dismantle the idea that these conditions look or act one specific way. By diversifying the face of EDS, we ensure that every patient—regardless of race, gender, or age—feels seen and validated.
Redefining Strength
"Strength is often quiet and invisible," as Jeevan Mann observes. The medical community often mistakes the ability to walk, work, or smile for a lack of severity. However, for those with EDS, these "ordinary" actions are often the result of immense, hidden effort.
Future Goals: From Survival to Thriving
Despite their daily battles, these individuals continue to pursue high-level goals. Whether it is Jeevan Mann’s quest to become a physician-scientist, Jacqueline Teti’s academic achievements despite severe health crises, or Krista Brack’s massive network of peer support, the goal for the EDS community is clear: moving beyond mere survival toward a future where treatment, understanding, and quality of life are not just aspirations, but guaranteed standards of care.
A Final Note
Living with EDS or HSD requires a radical commitment to finding joy in the small, manageable moments. It requires a community that refuses to accept the status quo of medical gaslighting and systemic neglect. As we look beyond Awareness Month, the call to action is clear: listen to the patients, fund the research, and acknowledge that the struggle, while invisible to the naked eye, is the most profound challenge these individuals face every single day.






