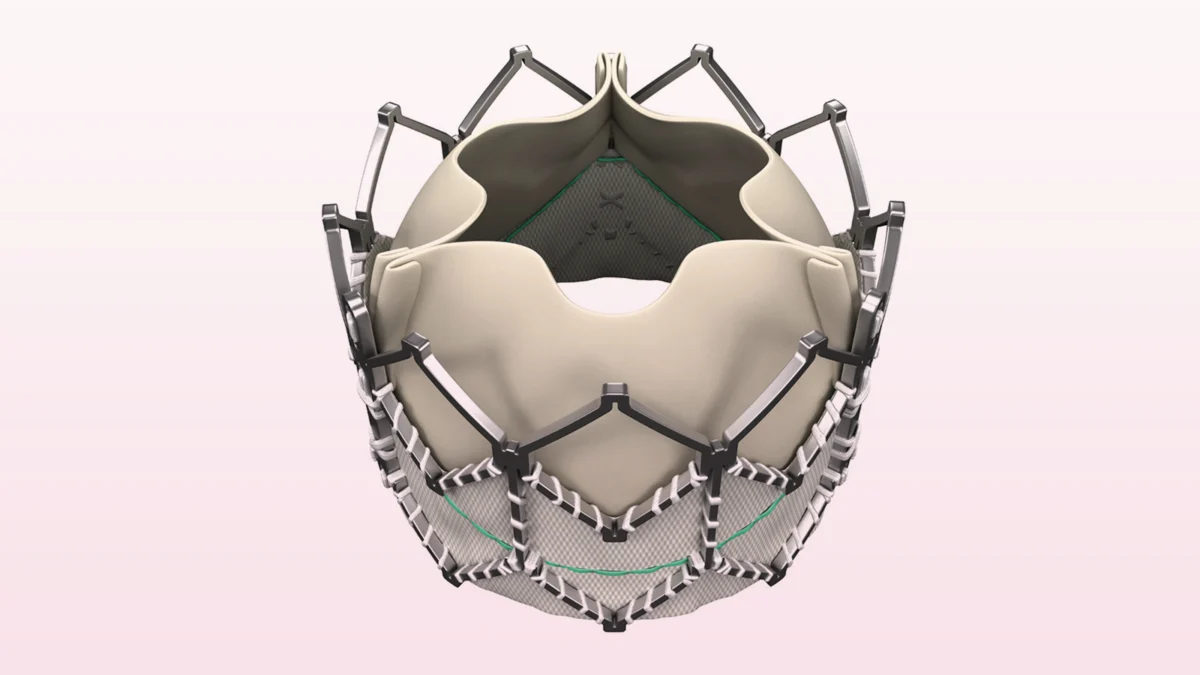
The landscape of cardiovascular medicine has been fundamentally reshaped by transcatheter aortic valve replacement (TAVR). Once a desperate, last-resort intervention for patients deemed too frail for open-heart surgery, the procedure has matured into a standard-of-care treatment for millions. However, as the field crosses the ten-year milestone, clinicians are finally gaining the longitudinal clarity required to evaluate the long-term durability and safety of these devices.
A dual release of findings published in the Journal of the American College of Cardiology has provided a sobering, yet optimistic, look at this journey. By comparing the outcomes of the early-generation Sapien XT device with the more refined Sapien 3, researchers have demonstrated that the "10-year TAVR result" is not a static metric, but a reflection of a rapidly iterating technological ecosystem.
Main Facts: A Tale of Two Generations
The primary takeaways from the recently published data center on the stark performance gap between device generations. In the landmark PARTNER 2A randomized trial, which evaluated the second-generation Sapien XT, long-term outcomes were undeniably disappointing. Researchers observed that all-cause mortality reached 86.1% in the TAVR group compared to 82.8% in the surgical cohort, a statistically significant difference that signaled early limitations in the technology.
Conversely, an observational analysis of the third-generation Sapien 3 valve yielded far more encouraging results. When compared against matched surgical controls, the Sapien 3 showed no significant difference in survival or the need for aortic valve reinterventions at the ten-year mark.
These findings underscore a critical narrative: the failures observed in the older cohort are largely attributed to the limitations of the era, including less precise valve sizing, a lack of routine CT-based procedural planning, and more invasive access routes. As the technology evolved, so too did the patient outcomes, effectively closing the performance gap between transcatheter and surgical approaches.
Chronology: The Maturation of a Procedure
To understand the current findings, one must look at the timeline of the PARTNER trials, which served as the crucible for modern TAVR practice.
- 2011: Enrollment begins for the PARTNER 2A trial. At this time, the Sapien XT was the state-of-the-art, and the medical community was still navigating the "learning curve" of TAVR implementation.
- 2014: The PARTNER 2 registry commences, reflecting the integration of the third-generation Sapien 3 valve. This period marked a shift toward more sophisticated patient screening and the adoption of systematic CT-based sizing.
- 2016–2024: As these patients reached the decade mark, researchers faced the monumental task of re-consenting patients and tracking vital status, a process complicated by the natural mortality rates of an elderly, high-risk population.
- 2026: The publication of the 10-year data confirms that the "first generation" of TAVR practice was a developmental phase, while the "second generation" (represented by the Sapien 3) has reached parity with surgery.
This chronology highlights that early TAVR was a pioneer’s game. The "disappointing" results of the XT device were a function of being the first to climb a steep mountain; the subsequent success of the Sapien 3 proves that the mountain has been successfully mapped.
Supporting Data: Examining the Disparities
The statistical weight of the PARTNER 2A study reveals exactly where the older-generation TAVR struggled. In the XT cohort, the incidence of aortic valve reinterventions hit 6.3%—significantly higher than the 1.6% observed in the surgical group. Furthermore, moderate or greater paravalvular regurgitation (leaking around the valve) occurred in 10.5% of TAVR patients compared to 0% in surgery.
The access route also played a decisive role in mortality. The study noted that patients who underwent TAVR via transapical (TA) or transaortic (TAo) routes—methods used when the traditional transfemoral (TF) route was blocked by peripheral vascular disease—suffered higher mortality. This is largely because these patients were inherently sicker and had a greater burden of systemic cardiovascular disease.
In contrast, the observational analysis of the Sapien 3 showed a much tighter alignment. After propensity score matching, all-cause mortality was a comparable 83.4% for TAVR and 82.3% for surgery. The reintervention rates also converged, with 2.0% for TAVR and 1.9% for surgery, confirming that the refinements in the Sapien 3 design and the improved procedural rigor of the operators were paying dividends.
Official Responses and Clinical Interpretation
The medical community has received these reports with a mix of academic caution and professional validation. Dr. Vinod Thourani, lead researcher of the PARTNER 2A trial, emphasized that the 10-year findings must be contextualized within the history of the procedure. He noted that the high rates of reintervention and leakage were "limitations of the Sapien XT device and the absence of routine CT-based sizing," which are now non-negotiable standards in current practice.
Dr. Aakriti Gupta of Cedars-Sinai Medical Center provided a poignant synthesis in her editor’s note, stating: "Read together, these reports show that there is no single ’10-year TAVR result.’ Long-term outcomes are shaped by the index procedure."
The editorial team, including Dr. Davide Capodanno and Dr. Kamil Bujak, praised the efforts to reach the 10-year milestone despite the logistical hurdles of long-term patient follow-up. They noted that while the data does not diminish the transformative power of TAVR, it serves as a "timely reminder that durability remains a central consideration as the field enters its second decade."
Implications: The Limits of Transcatheter Management
While the transition from Sapien XT to Sapien 3 has been a triumph, experts are now debating the "inherent limits" of the technology. Dr. Michael Borger, in his editorial for the Journal of the American College of Cardiology, raised a thought-provoking concern regarding the long-term performance of valves that are implanted within the calcified remnants of the native aortic valve.
Because TAVR generally involves crushing the native, calcified leaflets rather than excising them (as is done in surgery), there is a theoretical limit to how long these prosthetic leaflets can function under such mechanical stress. As TAVR moves into younger, lower-risk patient populations, the demand for "lifetime management" becomes paramount.
The industry is already responding to these concerns with newer platforms, such as the Sapien 3 Ultra and the Ultra Resilia, which are designed for better sealing and increased durability. The next great challenge will be the results of the PARTNER 3 trial, which will look at younger, lower-risk patients. If these patients show sustained outcomes at the ten-year mark, it will effectively cement TAVR as the definitive, lifelong solution for aortic stenosis.
Ultimately, the data from 2026 confirms a trajectory of continuous improvement. The "disappointment" of the past decade is the foundation of the current standard of excellence. As the field looks toward the next ten years, the focus will shift from simply ensuring the survival of the procedure to ensuring the lasting structural integrity of the valves themselves, confirming that the evolution of TAVR is far from over.