






The landscape of modern mental health care is currently undergoing a profound ideological schism. On one side stands the established biomedical model, which emphasizes chemical imbalances and pharmaceutical intervention; on the other stands a growing movement of critics, clinicians, and "survivors" of the system who argue that the current paradigm is not only failing but frequently causing irreparable harm.
In a recent, expansive two-part interview on the Psychophobia podcast, hosted by Dr. Michael Montgomery, investigative journalist and author Robert Whitaker delved into the systemic failures of contemporary psychiatry. Using the harrowing personal history of rock legend Stevie Nicks as a catalyst, Whitaker and Montgomery explored the "polypharmacy" epidemic, the lack of long-term evidence for multi-drug regimens, and the emerging international models that prioritize human connection over chemical suppression.
Main Facts: The Human and Systemic Cost of Over-Prescription
The centerpiece of the discussion revolves around the "lost years" of Stevie Nicks, whose experience serves as a high-profile cautionary tale. After successfully overcoming a cocaine addiction in the mid-1980s, Nicks sought psychiatric help for anxiety. She was prescribed Klonopin, a potent benzodiazepine. What followed was an eight-year period she describes as a "black hole," characterized by a loss of creativity, significant weight gain, and a total erosion of her "zest for life."
Whitaker uses Nicks’ story to illustrate a broader phenomenon: the transformation of patients into "chronic" cases through the very treatments intended to help them. The core facts presented in the discussion include:
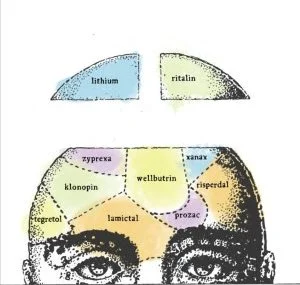
- The Polypharmacy Epidemic: The increasing clinical trend of prescribing multiple psychiatric medications simultaneously—a practice Whitaker asserts has "zero, zip" evidence from long-term, randomized controlled trials.
- The "Worst of the Worst" Fallacy: The case of Dr. Tony Stanton’s residential center demonstrates that even children labeled as the most difficult cases often show dramatic improvement once "de-prescribed" and allowed to re-engage with their environment.
- Global Alternatives: Countries like Norway and Israel are successfully implementing "medication-free" psychiatric wards and "Soteria" houses, which focus on social support rather than immediate sedation.
- The Failure of the Biomedical Narrative: Whitaker argues that the "chemical imbalance" theory has been largely debunked by the scientific community, yet it remains the primary marketing tool and clinical justification for lifelong medication.
Chronology: From Deinstitutionalization to the "Prozac Era"
To understand the current crisis, Whitaker provides a historical context for how the United States arrived at its current pharmacological impasse.
The 1950s-1970s: The First Wave
The introduction of Thorazine and the first generation of antipsychotics led to the "Great Deinstitutionalization." While this allowed patients to leave state hospitals, it replaced the "walls of the asylum" with "chemical straitjackets." However, during this period, medications were often seen as a "bridge" to help a patient through a crisis, rather than a lifelong necessity.
The 1980s: The Rise of the "Chemical Imbalance"
The 1980s marked a pivotal shift. With the publication of the DSM-III and the launch of Prozac, the psychiatric establishment began marketing the idea that mental distress was a purely biological issue—a "broken brain" that required a "chemical fix." It was during this era that Stevie Nicks was prescribed Klonopin. The medical community began to view anxiety and depression not as responses to life circumstances, but as permanent biological defects.
The 1990s-Present: The Polypharmacy Boom
As the efficacy of single-drug treatments began to wane in clinical trials, the industry shifted toward "adjunctive" therapies. If an SSRI didn’t work, a doctor might add a mood stabilizer; if that caused sedation, a stimulant might be added. This "cascading prescription" model became the norm, despite a lack of data on how these drug combinations interact over decades.
Supporting Data: The Evidence Gap in Long-Term Care
Whitaker’s critique is rooted in his extensive review of clinical literature, much of which he detailed in his landmark book, Anatomy of an Epidemic. During the podcast, he emphasizes the disparity between short-term "symptom reduction" and long-term "functional recovery."
The Benzodiazepine Trap
Benzodiazepines, like the Klonopin taken by Nicks, are intended for short-term use (two to four weeks). However, data suggests that long-term use leads to "down-regulation" of GABA receptors. This means the brain loses its natural ability to calm itself, creating a physical dependency that makes withdrawal excruciating. Nicks herself noted that it took three months in a hospital just to safely detox from the drug—a process she described as more difficult than quitting cocaine.
The Stanton Findings
The mention of Tony Stanton’s residential center highlights a critical data point: the "rebound" effect. Stanton found that when children were removed from polypharmacy environments and placed in a high-support, low-medication setting, their cognitive functions and emotional regulation improved significantly. This challenges the "standard of care" which suggests that more severe symptoms require more aggressive medication.
The International Success of Medication-Free Wards
In 2016, the Norwegian Ministry of Health mandated that all regional health authorities provide medication-free treatment options. Preliminary data from these wards suggests that patients who choose this route often achieve higher levels of social functioning and employment compared to those on traditional high-dose regimens. Similarly, Israel’s "Soteria" houses—minimalist, home-like environments for people experiencing psychosis—have shown that recovery is possible with minimal or no antipsychotic intervention.
Official Responses: The Psychiatric Establishment’s Defense
The critiques leveled by Whitaker and organizations like Mad in America have not gone unanswered by the American Psychiatric Association (APA) and the broader pharmaceutical industry.
The APA Position
The APA generally maintains that psychiatric medications are life-saving interventions. They argue that for many patients, particularly those with schizophrenia or severe bipolar disorder, medication is the "gold standard" that prevents suicide and total functional collapse. They often frame Whitaker’s work as "stigmatizing" necessary medical treatment, suggesting that his critiques might discourage vulnerable people from seeking help.
The Pharmaceutical Industry
Drug manufacturers point to FDA approval processes as proof of safety and efficacy. They argue that "polypharmacy" is a clinical necessity for "treatment-resistant" patients. From their perspective, the complexity of the human brain requires a multi-targeted approach, and the "cascading" prescriptions are a sign of doctors trying every available tool to alleviate suffering.
The Counter-Critique
Mainstream psychiatry often accuses critics of "cherry-picking" data. They suggest that while Stevie Nicks had a negative experience, millions of others lead productive lives because of benzodiazepines and antidepressants. They view the "medication-free" movement as a regressive step that ignores the biological realities of mental illness.
Implications: A Revolution of "Help" Over "Healing"
The conversation between Whitaker and Montgomery concludes with a radical but simple proposition for the future of mental health care. If the current model—focused on diagnosis and chemical correction—is failing, what replaces it?
The "Notecard" Philosophy
Whitaker suggests that the revolution in care doesn’t require a complex new medical model, but rather a shift in the fundamental question asked by clinicians. Instead of asking "What is wrong with you?" or "What is your diagnosis?", the question should be: "How can I be of help to you?"
This shifts the power dynamic from the doctor (the expert on the brain) to the patient (the expert on their own life). It prioritizes housing, social connection, purpose, and trauma processing over the management of neurotransmitters.
The Rise of "Mad in America" and Global Advocacy
The success of Whitaker’s platform, Mad in America, indicates a growing hunger for this alternative narrative. It has become a hub for "lived experience" stories, where individuals share how they reclaimed their lives after moving away from the medical model. This movement is increasingly influencing policy, as seen in the World Health Organization’s recent guidance on mental health, which emphasizes person-centered and rights-based care, moving away from the over-reliance on psychotropic drugs.
Final Outlook: Recovery as a "Conspiracy Theory"
Perhaps the most striking point made in the podcast is the idea that "recovery" and "hope" have become marginalized concepts in modern psychiatry. In a system where patients are often told they have a "chronic, lifelong illness," the idea that someone can fully recover and live a drug-free life is sometimes treated with skepticism, or as Whitaker puts it, as a "conspiracy theory."
The implications of the Whitaker-Montgomery dialogue are clear: the current trajectory of escalating polypharmacy is unsustainable. As more individuals like Stevie Nicks come forward with their stories of "lost years," and as international models prove that alternatives are viable, the psychiatric establishment may be forced to reckon with a simple truth: sometimes the most profound "treatment" is the restoration of the patient’s agency and the simple act of human presence.
The revolution, it seems, will not be a new drug, but a return to a philosophy of care that fits on a notecard.