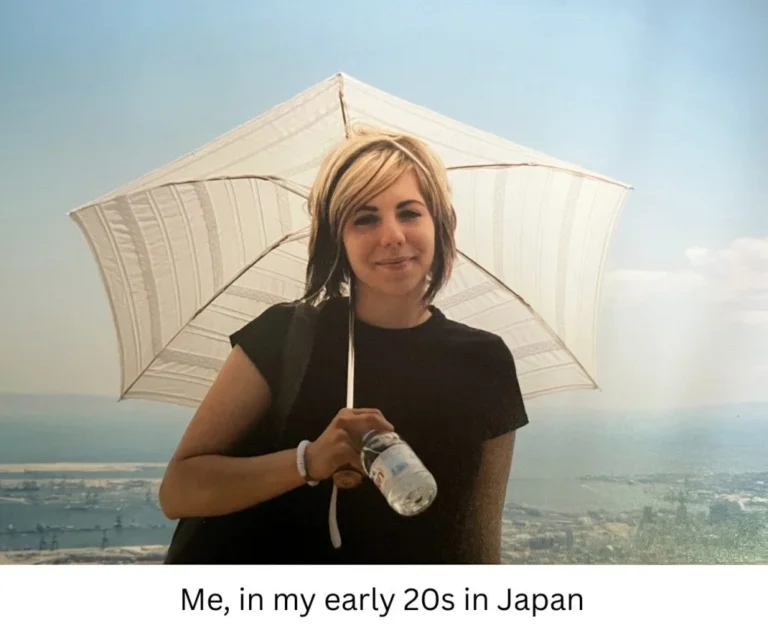









For Margaret Hvatum, a 70-year-old part-time computer science professor residing in Ladue, Missouri, life is measured in two distinct ways: the miles she logs on the pavement and the complex medical regimen required to keep her immune system functioning. A dedicated long-distance runner, Hvatum’s resilience was put to a grueling test this past January, when she completed a 5K, a 10K, a half-marathon, and a full marathon over four consecutive days. The distance covered was equivalent to traversing the length of Manhattan four times over.
Yet, as she crossed those finish lines, a different kind of race was beginning in the offices of her health insurance provider—a race against time and administrative red tape that would ultimately land her in a hospital bed. Hvatum, who lives with primary immunodeficiency, a condition that leaves her body uniquely vulnerable to infections, found herself caught in the gears of a system that prioritizes profitability over patient stability: the controversial process of prior authorization.
The Invisible Battle: Primary Immunodeficiency and the Cost of Care
Primary immunodeficiency is a lifelong struggle. For Hvatum, it is not merely a label; it is a daily, expensive reality. Diagnosed in 2005 after suffering through four separate bouts of shingles, Hvatum relies on a life-sustaining treatment known as immune globulin—specifically the product Hizentra. This medicine, comprised of antibodies harvested from donated blood plasma, provides the essential support her immune system lacks.
At her home in St. Louis, Hvatum manages her own care with clinical precision. She draws the viscous liquid into a syringe and loads it into a specialized apparatus—a device that resembles a child’s toy gun. By cranking a blue dial, she initiates a steady, slow infusion that travels through plastic tubing into her leg. It is a complex, delicate, and, above all, costly procedure. Without insurance coverage, a 28-day supply of this life-saving medication carries a staggering price tag of $8,141.94.
For over a decade, Hvatum’s insurance had covered this expense without issue. But when she switched to a new Medicare Advantage plan through Humana at the start of 2025, the stability she had cultivated for years evaporated.
Chronology of a Medical Crisis
The crisis did not emerge from a lack of medical necessity, but from a failure of administrative continuity.
- January 2025: Upon switching to a Humana Medicare Advantage plan, Hvatum received a cold notification: her "prior authorization prescription request" for Hizentra had been denied. Her previous insurer’s authorization did not transfer, triggering a bureaucratic freeze.
- Late January 2025: Deprived of her weekly doses, Hvatum’s health deteriorated rapidly. She developed a urinary tract infection. Despite it being a common ailment, her physician recognized that in an immunocompromised patient, the infection could escalate into a systemic crisis. She was admitted to the emergency department.
- January 30, 2025: What began as an ER visit turned into an overnight hospital stay. The bill arrived at $18,000, which Humana promptly denied, claiming her condition did not reach the threshold of "medical necessity" for hospital care.
- February 2025: After a grueling appeal process, Humana reversed the denial for her medication, but only with an expiration date at the end of the year, ensuring the battle will eventually repeat.
- March 2025: Hvatum suffered a stroke. Once again, Humana denied the subsequent hospital stay, arguing it wasn’t reasonable to expect a two-night stay for a "small stroke." This denial was eventually overturned, but only after two weeks of appeals.
The Mechanics of Denial: Data and Discrepancies
Hvatum’s experience is not an anomaly; it is a statistical probability. According to data from KFF, Medicare Advantage plans processed nearly 53 million prior authorization requests in 2024. That figure averages out to approximately two reviews for every single person enrolled in the program.
The business model behind these denials is transparent to health policy experts. Dr. Carrie Graham, director of the Medicare Policy Initiative at Georgetown University’s Center on Health Insurance Reforms, notes that the structure of Medicare Advantage creates a perverse incentive. The government pays insurers a fixed monthly sum per enrollee. "They make a profit if the care that person receives in that year is less than the amount they receive," Dr. Graham explains. Consequently, delaying or denying care is not merely an administrative bottleneck; it is a core component of the profit margin for many insurance giants.
With over 35 million Americans enrolled in Medicare Advantage—a group that includes half of all eligible beneficiaries—the scale of this impact is massive. Humana and UnitedHealth Group control nearly half of this market, giving them outsized influence over how millions of patients access care.
Official Responses and the Pledge of Reform
The death of UnitedHealthcare CEO Brian Thompson last year ignited a national conversation regarding the hostility of the insurance industry’s administrative hurdles. In response to public outcry and mounting pressure, the nation’s largest insurers, including Humana, signed a pledge to modernize the prior authorization process.
The commitments included promises to reduce the number of services requiring prior authorization and to honor existing authorizations for 90 days when patients switch plans. However, when tested by the reality of Hvatum’s situation, these promises proved hollow.
Mark Taylor, a spokesperson for Humana, clarified that the pledge to honor existing authorizations applies only to "medical services," explicitly excluding prescription medications like Hizentra. While Humana declined to comment on the specifics of Hvatum’s case—even with her waiver of privacy—they maintained that their process serves as a "check and balance" to ensure safety and taxpayer efficiency. In July 2025, the company announced it would remove one-third of prior authorization requirements for outpatient services, labeling the move as an effort to make the system "faster and more seamless."
For Hvatum, these statements are a day late and a dollar short. "They love to send you the denials fast," she remarked regarding her experience with the company’s turnaround times. "Approvals take longer."
Implications for the Future of Healthcare
The burden of this system falls squarely on the shoulders of the patient. Dr. Graham emphasizes that while the system is designed to be exhausting, the data suggests that persistence pays off. In 2024, 81% of appealed Medicare Advantage denials were partially or fully overturned. Yet, the high percentage of reversals indicates that the initial denials are often baseless, serving as a deterrent to keep patients from seeking the care they are entitled to.
For Hvatum, the psychological and physical toll has reached a breaking point. Her home is filled with the physical manifestations of her dedication to health: trophies, medals, and ribbons from years of running, hanging like drapery in her kitchen. She views her athleticism as a partnership with her medical care. "I have done everything I possibly can to be healthy," she says, wearing a T-shirt that reads, ‘If found on ground, please drag across the finish line.’
She has now switched to a different medication, but the stability of her future remains in question. Discouraged by the American healthcare landscape, she and her husband are exploring the possibility of moving to Norway, where her husband holds citizenship and universal healthcare is a guaranteed right, not a battle to be won.
As the industry continues to make promises of reform, Hvatum’s story serves as a stark reminder of the human cost of the "prior authorization" paradigm. When a system is designed to prioritize the prevention of payment over the prevention of illness, the most vulnerable patients are the ones left running a race they can never win. Whether through increased federal regulation or a fundamental shift in insurance accountability, the message from patients like Hvatum is clear: the current model of managed care is failing those who need it most.