As Ehlers-Danlos Syndrome (EDS) Awareness Month draws to a close, the medical community and the public at large are left with a critical question: how much of what we think we know about connective tissue disorders is actually grounded in reality?
Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorder (HSD) are often relegated to the sidelines of public health discourse, dismissed as rare, "bendy" anomalies. However, for the millions living with these conditions, the reality is a complex, systemic battle that consumes thousands of hours of life and energy each year. To challenge the pervasive stigma surrounding these conditions, we turn to the lived experiences of four individuals who navigate the intersection of chronic pain, medical gaslighting, and advocacy. By examining their journeys, we can begin to dismantle the myths that have long hindered proper diagnosis and empathetic care.

Main Facts: The Invisible Landscape of Connective Tissue Disorders
EDS and HSD are not merely issues of joint hypermobility; they are systemic conditions that affect the body’s connective tissue—the "glue" that holds everything together. Because connective tissue is found in blood vessels, skin, organs, and nerves, the symptoms are wide-ranging and often debilitating.
The core challenge lies in the "invisible" nature of these diseases. Patients frequently appear healthy, leading to skepticism from friends, employers, and, most alarmingly, medical professionals. This gap between the physical reality of the patient and the external perception creates a cycle of trauma, diagnostic delay, and social isolation. On average, patients often wait decades for a formal diagnosis, spending several hours every day simply managing symptoms, navigating insurance, and coordinating complex care for an array of comorbidities like Mast Cell Activation Syndrome (MCAS), Dysautonomia (POTS), and gastrointestinal dysfunction.
Chronology of Struggle: The Road to Diagnosis
The path to an EDS or HSD diagnosis is rarely linear. It is a grueling, multi-year odyssey characterized by missed signals and misdiagnoses.
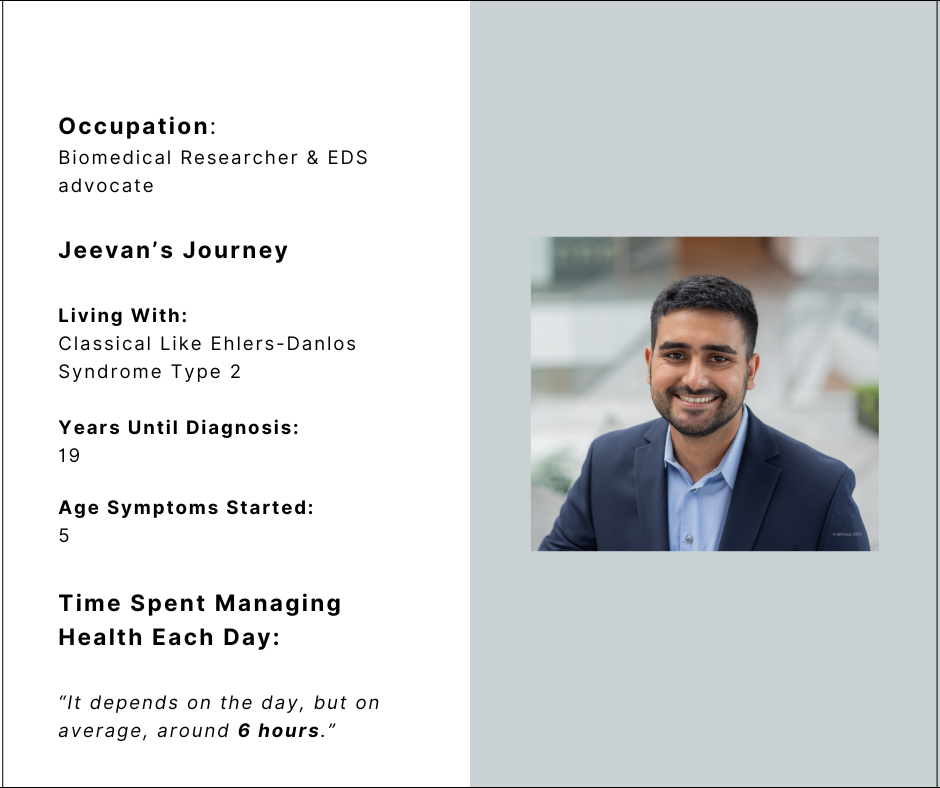
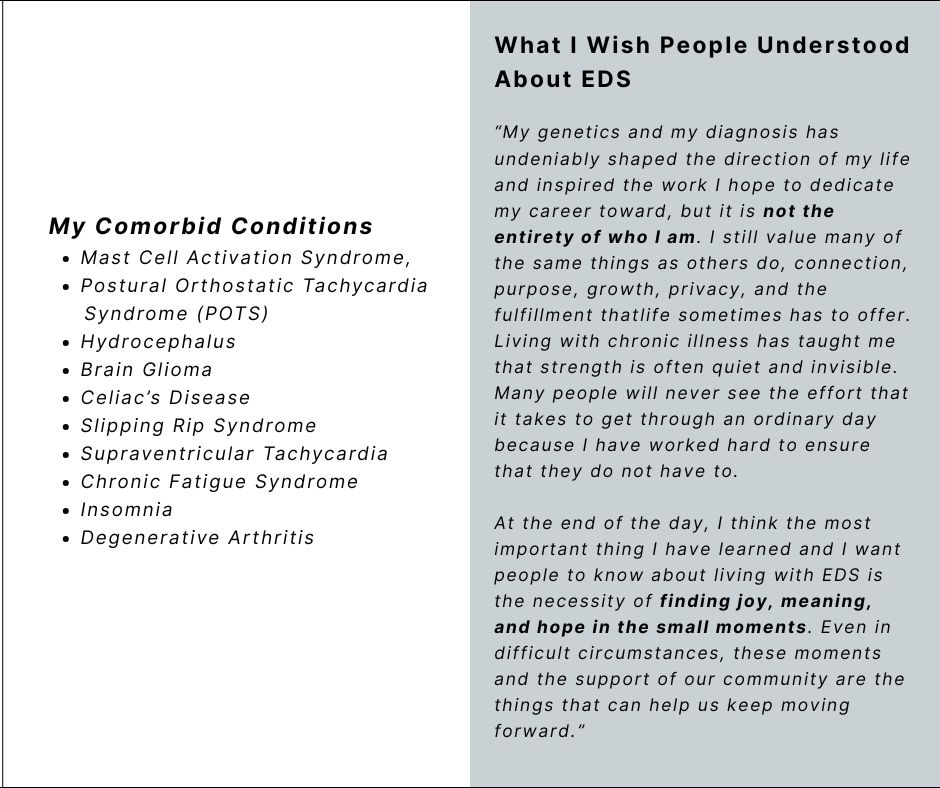
- Jeevan Mann (Classical-like EDS Type 2): Symptoms began at age five, yet it took 19 years to receive a diagnosis. For Jeevan, who now works as a biomedical researcher, the journey was defined by years of searching for answers while managing complex issues like hydrocephalus and brain glioma.
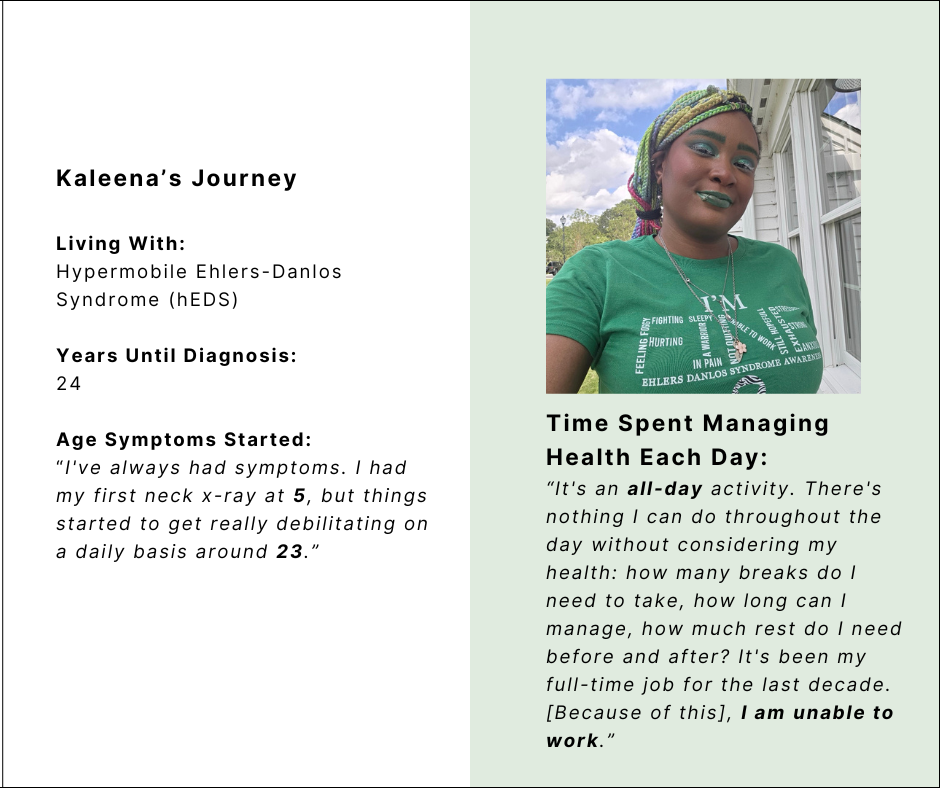
- Kaleena Deshawn (hEDS): Kaleena’s story highlights the systemic barriers in healthcare. With symptoms starting in childhood, she underwent her first neck X-ray at age five. It took 24 years to reach a diagnosis, during which time her health became a "full-time job," eventually rendering her unable to maintain traditional employment.
- Krista Brack (Classical EDS): Krista’s experience underscores the danger of the current diagnostic model. Suffering from birth, she waited 30 years for a diagnosis. During those three decades, she faced a cascade of severe complications, including tethered cord syndrome and craniocervical instability, often being left without support in emergency rooms.
- Jacqueline Teti (HSD): With symptom onset at age 16, Jacqueline navigated 21 years of uncertainty. Her story highlights that even after reaching academic and professional milestones, the daily reality of managing systemic dysfunction—including internal jugular vein compression—remains a persistent, labor-intensive burden.
Supporting Data: The Daily Cost of Chronic Illness
To understand the severity of these conditions, one must look at the time investment required for basic survival. For the individuals spotlighted here, "managing health" is not an occasional task; it is a rigid, mandatory daily schedule.
| Individual | Time Spent Daily on Health | Primary Struggle |
|---|---|---|
| Jeevan Mann | ~6 Hours | Balancing research goals with systemic pain. |
| Kaleena Deshawn | All-day activity | Energy conservation and pacing. |
| Krista Brack | 6 Hours | Navigating life-threatening ER mistreatment. |
| Jacqueline Teti | 3-4 Hours | Managing appointments and PT alongside work. |
These figures represent a "lost economy" of time—hours that would otherwise be spent on career advancement, social connection, or personal fulfillment. Furthermore, the presence of comorbidities such as Celiac’s disease, Scoliosis, and Chronic Fatigue Syndrome adds a layer of complexity that complicates treatment and recovery.
Official Perspectives and The Myth-Busting Initiative
The narratives of these four individuals serve as a direct rebuttal to the most common myths plaguing the EDS community.
Myth 1: "Men Can’t Have EDS"
Jeevan Mann’s journey serves as a powerful testament that EDS does not discriminate by gender. The outdated notion that EDS is exclusively a "female" condition has led to massive underdiagnosis in men. By being vocal about his diagnosis, Jeevan is not only advocating for better awareness but also helping to normalize the presence of connective tissue disorders across all gender identities.
Myth 2: "EDS Doesn’t Affect All Backgrounds"
Kaleena Deshawn’s experience reveals a disturbing trend: the perception of EDS as a "European disease." This bias has created significant barriers for Black patients and people of color, who are frequently dismissed when they report their symptoms. Kaleena notes that support groups themselves have often been "white spaces," further alienating patients who are already struggling to be heard by the medical establishment.
Myth 3: "EDS is Just Being ‘Bendy’"
Krista Brack’s testimony shatters the trivialization of the condition. While joint hypermobility is a hallmark, it is the secondary complications—the organ failure, the spinal issues, the neurological dysfunctions—that pose the greatest threat. As Krista notes, she is in pain even when she is smiling; the "bendy" label fails to capture the systemic nature of the chronic pain she lives with every day.
Myth 4: "If You Were Actually Sick, You Would Look Sick"
Jacqueline Teti’s academic and professional success, achieved while battling severe dysautonomia, proves that visible health is not synonymous with physical well-being. The "look sick" myth forces patients to perform their pain, creating a secondary burden of proof that consumes their remaining energy.
Implications: The Path Forward
The implications of these lived experiences are clear: the current medical and social infrastructure is failing those with EDS and HSD. The lack of awareness in emergency departments is not just an inconvenience; it is a life-threatening failure.
Advocacy and Education:
The work being done by individuals like Krista Brack (leading support groups) and Jeevan Mann (conducting biomedical research) is the blueprint for future progress. However, the burden of advocacy should not rest solely on the shoulders of the patients.

Institutional Reform:
Medical schools must integrate the study of hereditary connective tissue disorders into core curricula. Emergency response teams need updated protocols for patients with systemic hypermobility to ensure that conditions like subluxations or POTS-related crises are handled with appropriate care rather than skepticism.
Cultural Empathy:
Finally, there is a societal need to redefine "strength." As Jeevan Mann beautifully articulates, "Strength is often quiet and invisible." We must stop measuring disability by what we see on the surface and start acknowledging the immense labor—the quiet, unseen hours—that patients put into simply existing.
As we move beyond May, let these stories serve as a catalyst for change. The goal is not just to provide awareness, but to foster an environment where patients are believed, supported, and treated with the dignity they deserve. Whether it is through advancing physician-scientist training, as Jacqueline Teti and Jeevan Mann hope to do, or by building robust, inclusive support networks, the community is rising. It is time for the rest of the world to catch up.
This article was compiled by the editorial team at Chronic Pain Partners, honoring the voices of those who continue to fight for better care, validation, and a future where EDS/HSD are understood as the complex, multisystemic conditions they truly are.