









For many women in their late 40s and early 50s, the transition into menopause is often marked not by a single, dramatic event, but by a slow, insidious erosion of cognitive clarity. It is a sensation often described as living with a "pile of sludge" in the brain—a persistent haze that obscures names, stunts productivity, and renders once-simple tasks, like recalling the name of a favorite restaurant, an insurmountable challenge.
While society frequently frames menopause through the narrow lens of hot flashes and reproductive cessation, a growing body of research suggests that this life stage represents a profound neurological and physiological transition. For millions, the "brain fog" and emotional turbulence associated with this period are not merely symptoms of stress or aging; they are clinical indicators of a hormonal shift that, when left unaddressed, can significantly diminish quality of life.
The Anatomy of the Menopausal Shift
Menopause is not a disease; it is a natural, albeit complex, life transition. Medically, it is defined as the point reached 12 consecutive months after a woman’s final menstrual period. However, the years leading up to this—perimenopause—and the years following, involve a dramatic recalibration of the endocrine system.
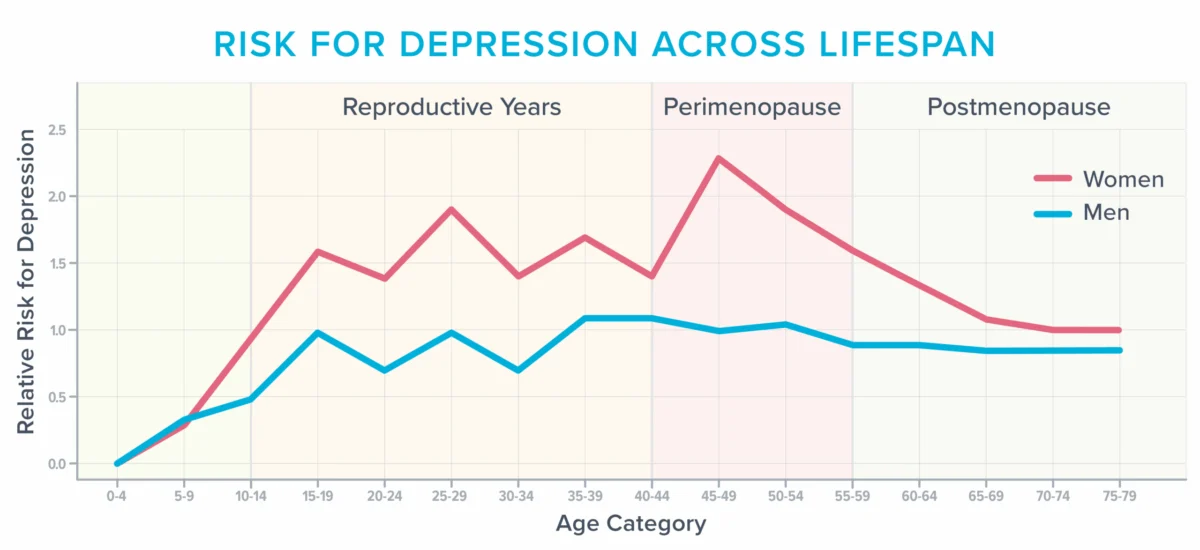
As estrogen and progesterone levels fluctuate and ultimately decline, the systemic impact is vast. The American College of Obstetricians and Gynecologists reports that approximately 40 percent of women experience increased irritability, mood swings, anxiety, and profound fatigue during this transition. This period is statistically one of the most vulnerable windows in a woman’s life for the onset or exacerbation of depression, particularly for those with a prior history of the condition.
The diagnostic challenge lies in the "symptom overlap." The criteria used by many clinicians to diagnose clinical depression—fatigue, sleep disturbances, cognitive difficulty, and loss of interest—are identical to the hallmark symptoms of menopausal vasomotor instability.
A Chronology of Confusion: Seeking Answers
For many, the search for relief is a frustrating journey through a "revolving door" of medical specialists. The narrative of the modern woman often mirrors this cycle: initial symptoms like brain fog and lethargy are met with prescriptions for antidepressants or sleep aids, which often fail to address the root cause.
In many cases, the disconnect stems from a lack of specialized training. Surveys indicate that up to 80 percent of medical residents feel "barely comfortable" discussing menopause, and few residency programs provide comprehensive education on the subject. Consequently, many women spend years misdiagnosed, feeling like a "zombie" on ineffective medication, when their symptoms are actually the result of a physiological hormonal deficit that could be managed with targeted hormone therapy.
The Physiological Basis: Vasomotor Symptoms and the Brain
For decades, hot flashes and night sweats were dismissed as minor inconveniences. Modern neuroscience has revised this view. These "vasomotor symptoms" involve the constriction and dilation of blood vessels, regulated by the hypothalamus—the brain’s internal thermostat. When estrogen levels drop, the hypothalamus can become hyper-reactive, signaling the body to shed heat even when it is not overheating.

Crucially, researchers have identified a direct link between the frequency of these episodes and changes in brain health. Magnetic resonance imaging (MRI) studies have revealed that women who suffer from frequent, severe hot flashes often exhibit higher levels of "white matter intensities"—small, patchy lesions in the brain. Once thought to be a benign sign of aging, these lesions are now considered predictive of future cognitive decline and increased stroke risk.
Furthermore, night sweats—even those that do not result in overt perspiration—cause frequent, micro-arousals during sleep. These interruptions prevent the brain from performing vital maintenance, such as toxin clearance and memory consolidation. This chronic sleep deprivation degrades the hippocampus (the center for learning and memory) and keeps the amygdala (the center for emotional regulation) in a state of high alert, contributing to the "rage" or "anxiety" often reported by women in this life stage.
Supporting Data: Why "Defensive Medicine" Prevails
The hesitancy among many healthcare providers to prescribe Menopausal Hormone Therapy (MHT) is often rooted in "defensive medicine." This stems from the fallout of older, widely publicized studies that linked hormonal intervention to increased risks of breast cancer and stroke.
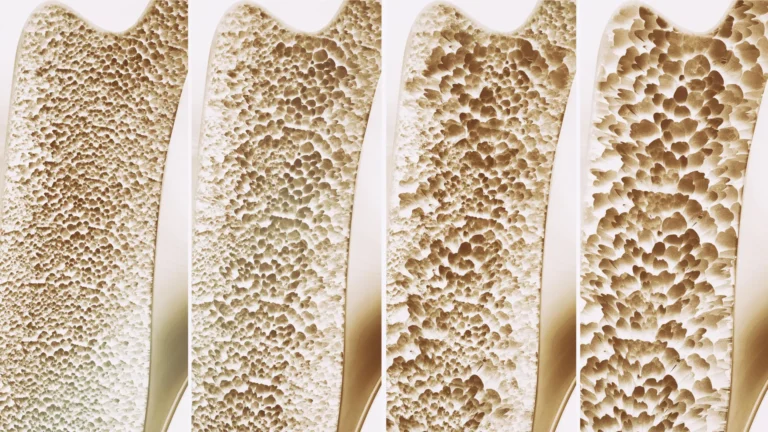
However, contemporary clinical consensus has shifted. Experts, including those aligned with the Menopause Society, argue that for healthy women under the age of 60 who are within 10 years of the onset of menopause, the benefits of MHT—including protection against osteoporosis and potential cognitive preservation—far outweigh the risks. The decision to forgo treatment based on outdated data, or to substitute antidepressants for hormone therapy, often ignores the fundamental physiology of the patient.
Implications for Patient Advocacy
The path to better health during menopause requires a shift toward active patient advocacy and the adoption of "shared decision-making" models. To navigate the medical system effectively, patients should:
- Seek Specialized Care: Look for practitioners certified by the Menopause Society.
- Document Everything: Use tracking tools to record the frequency of hot flashes, sleep quality, and mood fluctuations. Specific data—such as "I wake five times a night"—is more actionable than general complaints.
- Demand Data-Driven Discussions: Engage in frank conversations about the risks and benefits of MHT versus alternatives. Ask, "Based on my medical history, what are the actual risks compared to the known risks of chronic sleep deprivation?"
Holistic Strategies: Beyond Hormones
While MHT is a powerful tool, it is most effective when paired with lifestyle foundations. Managing the menopausal transition requires a multi-pronged approach:
- Nutritional Support: While no specific diet cures vasomotor symptoms, Mediterranean-style eating patterns rich in whole grains, legumes, fish, and nitrate-rich vegetables (like beets) support vascular health and blood flow to the brain.
- Exercise Optimization: The "more is better" approach to exercise can be counterproductive during menopause. High-intensity training, if not balanced with adequate recovery, can spike cortisol and exacerbate fatigue. Instead, focus on a blend of Zone 2 cardio and strength training, with flexibility for gentle movement on days when sleep has been poor.
- Cognitive Behavioral Therapy for Insomnia (CBT-I): This is the gold standard for managing sleep disturbances. It provides the tools to regulate sleep architecture, regardless of hormonal fluctuations.
- The Power of "No": Perhaps the most significant lifestyle change is the strategic reduction of life stress. Menopause often coincides with the peak of professional and caregiving responsibilities. Evaluating one’s capacity and setting rigid boundaries is not just a mental health preference—it is a physiological necessity for recovery.
- Supplements and Sunlight: Creatine monohydrate (5–7 grams daily) has shown promise in supporting brain function and mitigating mental fatigue. Additionally, morning sunlight exposure remains the most effective tool for resetting the circadian rhythm, which helps stabilize both energy levels and sleep quality.
The Hidden Opportunity
Ultimately, the transition into menopause forces a reckoning with how women spend their most limited resource: their energy. The "fog" often acts as an unwanted, yet loud, signal that the previous mode of living—characterized by over-commitment and under-recovery—is no longer sustainable.
By reframing this life stage as a transition rather than a decline, women can reclaim their agency. With the right medical intervention, a commitment to fundamental health habits, and the courage to simplify their lives, the years following menopause can be a time of renewed clarity and purpose. The "sludge" does not have to be a permanent state; it is often merely the body’s way of demanding a new way of existing.