






In December 2025, the antidepressant gepirone, marketed under the brand name Exxua, became commercially available to the American public. To a casual observer, the launch of a new psychiatric medication represents a triumph of medical innovation. However, beneath the surface of its commercial release lies one of the most contentious approval histories in the history of the U.S. Food and Drug Administration (FDA).
Exxua’s journey to the pharmacy shelf was marked by four formal rejections, a 9-to-4 vote against approval by an independent scientific advisory committee, and a clinical record where 11 out of 13 efficacy trials failed to meet their primary objectives. Despite this, the drug is now being marketed at a price point of approximately $1,788 per month, with projected annual revenues expected to reach $165 million by 2029.
The approval has reignited a fierce debate over the FDA’s standards for "substantial evidence" of efficacy and the transparency of the information provided to prescribing physicians. A recent exposé in JAMA Psychiatry by Erick H. Turner, a former FDA reviewer and professor emeritus at Oregon Health and Science University, suggests that the case of gepirone is not an isolated incident, but rather a symptom of a systemic "regulatory corruption" that prioritizes industry interests over clinical clarity.
Main Facts: A Statistical Paradox
The central controversy surrounding Exxua involves the sheer volume of negative data that the FDA ultimately set aside to grant approval. Under the Federal Food, Drug, and Cosmetic Act, a drug must demonstrate "substantial evidence" of effectiveness, typically interpreted as at least two "adequate and well-controlled" positive trials.
Gepirone technically met this minimum requirement, but only after nearly four decades of testing. Out of 13 total trials conducted, 11 failed to show that the drug was more effective than a placebo. Furthermore, in several of those failed trials, gepirone performed significantly worse than existing, older antidepressants like Prozac (fluoxetine) and Paxil (paroxetine).
The discrepancy between the drug’s performance and its approval highlights a significant gap in public and professional understanding of the FDA’s role. According to Turner’s research:
- Public Perception: Nearly 50% of U.S. adults mistakenly believe the FDA only approves "extremely effective" drugs.
- Physician Misconception: 70% of surveyed physicians believe the FDA requires clinical trial results to show both statistical and clinical significance.
- Comparative Efficacy: 73% of doctors believe a new drug must be at least as effective as existing treatments for the same condition to gain approval.
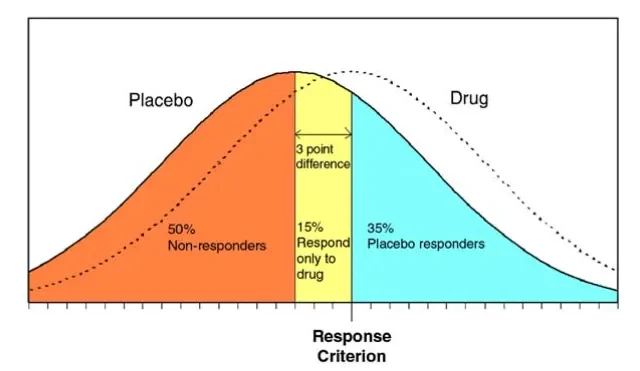
In reality, the FDA does not require a drug to be better than—or even equal to—existing treatments. It only requires that a drug "beats" a sugar pill (placebo) in two trials, regardless of how many other trials fail.
Chronology: Forty Years of Rejection
The timeline of gepirone’s development is a saga of corporate persistence and regulatory shifts.

- 1986–1993: Originally synthesized by Bristol-Myers Squibb, the drug was eventually abandoned and the rights sold to Fabre-Kramer.
- 1999–2002: Organon, partnering with Fabre-Kramer, submitted the first New Drug Application (NDA). The FDA issued a "Refuse to File" letter, citing methodological flaws and a lack of evidence.
- 2003–2004: A resubmission was met with a "Not Approvable" letter. The FDA noted that the company had allegedly manipulated data in a maintenance trial by reclassifying relapsed patients after the study had been "unblinded."
- 2007: After Fabre-Kramer regained full rights, a fourth NDA—incorporating 13 trials—was rejected. The FDA stated the data simply did not prove the drug worked.
- 2015: Following a formal dispute resolution request, an FDA advisory committee of independent experts reviewed the evidence. They voted 9 to 4 against approval, citing insufficient evidence of efficacy.
- 2016: In a surprising reversal, John Jenkins, then Director of the FDA Office of New Drugs, granted an appeal. He argued that the FDA should focus on the two positive trials and discount the negative ones.
- 2023–2025: Supported by Janet Woodcock, then Director of the Center for Drug Evaluation and Research, the drug received final approval in September 2023 and hit the market in late 2025.
Supporting Data: The "Jenkins Pivot" and Meta-Analysis
The approval of Exxua hinged on a specific reinterpretation of the failed data, led by John Jenkins. The primary mechanism for this reversal was a "meta-analysis" provided by the drug’s sponsor, Fabre-Kramer.
The Problem of "False Positives"
FDA staff experts had previously warned that if you run enough trials, two might eventually return positive results by sheer chance—a phenomenon known as the "multiplicity problem." These experts concluded that the probability of gepirone’s two positive trials being "false positives" was unacceptably high.
Statistical Manipulation
To counter this, Fabre-Kramer conducted a meta-analysis that selectively excluded more than half of the failed studies. By removing these "failed" trials from the calculation, the company was able to show a slight statistical separation from the placebo. Even then, the drug only improved depression scores by an average of 1.32 points on the Hamilton Depression Rating Scale (HAMD-17). Most clinicians consider a 2-point difference to be the bare minimum for "clinical significance."
The "Failure is Normal" Argument
Perhaps the most striking justification for the approval came from Jenkins himself. He argued that since existing, approved antidepressants fail to beat the placebo in about 50% of their trials, a high failure rate should not disqualify a new drug. Jenkins stated, "It is not uncommon for effective anti-depressants to fail to beat placebo… that would not necessarily preclude approval."
This logic suggests a regulatory environment where the "bar" for efficacy is not set by the drug’s actual performance, but by the historically low performance of the class of drugs it belongs to.
Official Responses: Internal Friction at the FDA
The internal documents released via the JAMA Psychiatry report reveal a deep divide within the FDA’s upper echelons. While leadership moved toward approval, senior reviewers like Deputy Director Robert Temple remained staunchly critical.
Temple pointed out that in four specific studies, gepirone was tested against "active controls" (existing antidepressants). In those studies, the existing drugs worked, but gepirone did not. Temple wrote that the negative trials "raise considerable doubts about the effectiveness of gepirone in the acute or sustained treatment of depression."
Despite these internal warnings and the 9-4 "No" vote from the external advisory committee, Jenkins and Janet Woodcock moved forward. Their rationale was that the drug offered a "different" mechanism of action (a 5HT1a agonist) that might have fewer side effects, such as weight gain or sexual dysfunction. However, critics argue that a lack of side effects is irrelevant if the drug does not effectively treat the primary condition.

Implications: The Transparency Crisis
The commercial availability of Exxua raises urgent questions about the ethics of drug labeling and informed consent.
Misleading Labels
The current FDA-approved product label for Exxua states that the drug "was evaluated in two eight-week randomized, double-blind, placebo-controlled… studies." It makes no mention of the 11 failed trials. It does not disclose that the drug performed worse than Prozac in comparative studies.
Erick Turner argues that this omission is a direct threat to the integrity of medical practice. "Provided with this information [the current label], clinicians may understandably assume that the drug worked in all trials conducted," Turner writes. Because these labels inform secondary databases like UpToDate and Micromedex, the "sanitized" version of the drug’s history becomes the standard of care.
The Financial Cost
With a monthly price tag of nearly $1,800, Exxua is significantly more expensive than the generic SSRIs it failed to outperform in clinical trials. For patients and insurance payers, this represents a massive expenditure for a treatment that an independent panel of experts concluded was not proven to be effective.
The Call for Reform
The gepirone controversy has led to renewed calls for structural changes at the FDA. Proposed reforms include:
- Mandatory Transparency: Requiring product labels to list the total number of trials conducted, including failed ones.
- Advisory Committee Weight: Mandating that the FDA abide by the votes of its scientific advisory committees, or provide a public, high-threshold justification for overrule.
- Clinical Significance Standards: Moving beyond simple "statistical significance" (p < 0.05) to require "clinical significance"—actual, meaningful improvement in a patient’s life.
As Exxua enters the medicine cabinets of thousands of Americans, the story of its approval remains a cautionary tale of how regulatory maneuvers can transform a four-time rejected drug into a multimillion-dollar commercial product, all while keeping the most critical data out of the sight of the doctors who prescribe it.