







For many, the phrase "my ostomy bag saved my life" is synonymous with emergency surgery for inflammatory bowel disease (IBD), acute infections like diverticulitis, or the removal of cancerous tumors. These conditions carry clear, quantifiable pathology—visible evidence that makes the surgical decision relatively straightforward. However, for those living with Ehlers-Danlos syndrome (EDS), the path to an ostomy is often paved with ambiguity, gaslighting, and a medical system ill-equipped to handle invisible, systemic dysmotility.
This is the story of a two-year journey—a "stoma-versary"—that highlights how one woman moved from a lifetime of debilitating gastrointestinal (GI) distress to finding liberation through a procedure often misunderstood by both patients and providers.
The Invisible Burden: EDS and the Gastrointestinal Tract
Ehlers-Danlos syndrome is a group of hereditary connective tissue disorders. While often stereotyped as "just a bendy joint disorder," EDS is fundamentally multisystemic. Connective tissue acts as the scaffolding for the human body; when that scaffolding is structurally compromised, it impacts skin, blood vessels, organs, and—crucially—the digestive system.
For the author, Tayler Goectau, the manifestations were gastrointestinal. From the hallways of elementary school, where waves of intense abdominal pain were a constant companion, to the isolation of college life, where the fear of bathroom emergencies tethered her to her home, the struggle was all-consuming. Despite seeking help, she was frequently dismissed, told her symptoms were "just constipation" or psychological in origin.
A Chronology of Chronic Suffering
The progression from childhood discomfort to a life-altering surgery was not linear; it was a grueling, decades-long battle against a medical establishment that struggled to connect the dots.
- The Early Years: Persistent, unexplained abdominal pain that defied traditional pediatric GI explanations.
- The Escalation: By early adulthood, symptoms reached a breaking point. Conventional treatments—laxatives, dietary modifications, and motility agents—failed to provide relief. The condition became so severe that it prevented basic social and professional functioning.
- The Diagnostic Gap: The lack of awareness regarding how EDS affects intestinal motility led to years of misdiagnosis. It wasn’t until a specialist looked beyond standard testing that the underlying issues—visceroptosis (the abnormal downward displacement of abdominal organs) and severe dysmotility—began to surface.
- The Cascade of Testing: Through a series of specialized imaging and diagnostic procedures, Goectau had to act as her own advocate, often guiding radiologists and surgeons toward the correct diagnostic protocols.
- The Surgical Turning Point: After an initial stoma creation in 2024 provided immediate relief, a total colectomy was performed one year later to remove the "dead weight" of a non-functioning colon.
The Anatomy of an Ostomy
To understand the gravity of this transition, it is necessary to define the procedure. An ostomy is a surgical opening (a stoma) in the abdominal wall, which allows waste to exit the body into an external pouch, bypassing the traditional route.

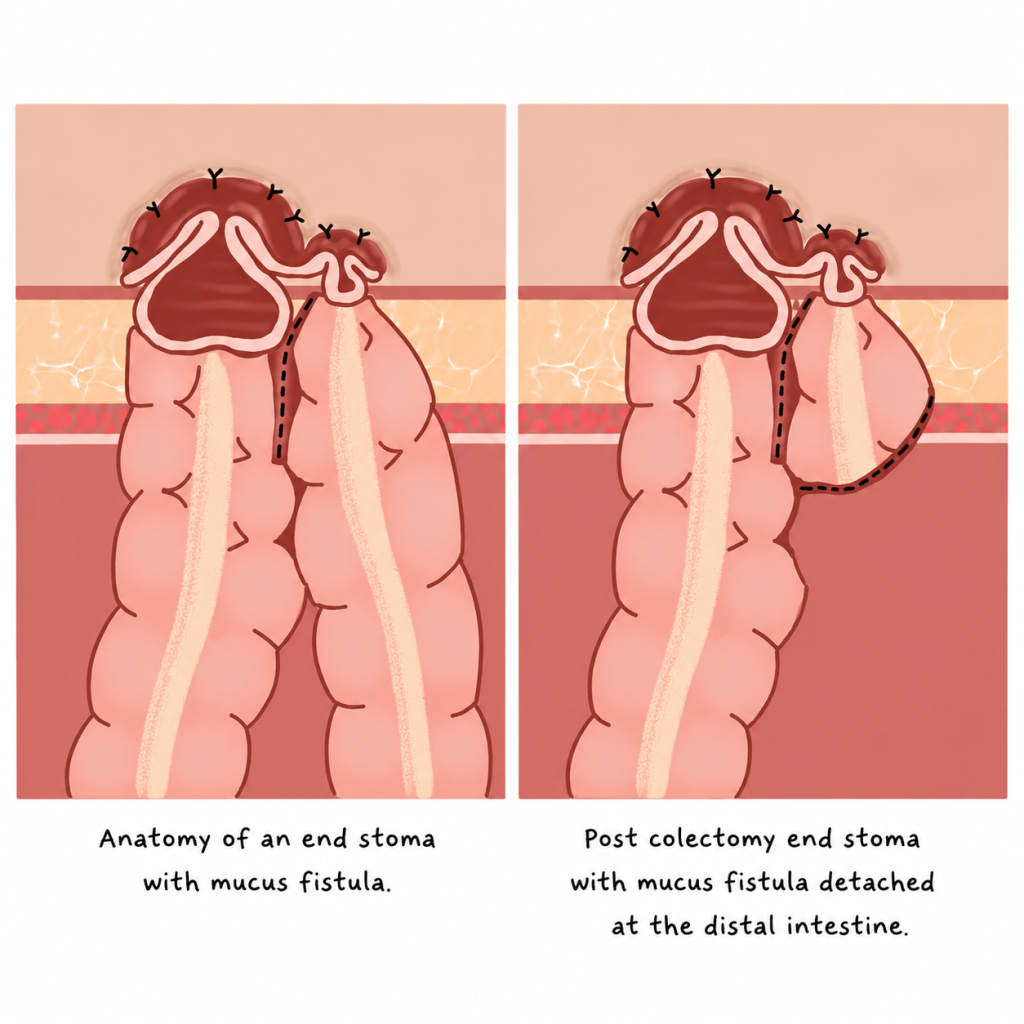
Goectau’s procedure was an end ileostomy, where the small intestine is brought to the surface after the removal of the colon. This differs from a loop ostomy, which is typically temporary and involves a loop of the bowel. Because the large intestine remained in the body for a period, she underwent a procedure involving an end stoma with a mucus fistula. This technical precision was essential for a body whose connective tissue fragility made recovery inherently complex and non-linear.
The Psychological Toll: Self-Gaslighting and the Decision
The decision to undergo a permanent ostomy is not merely surgical; it is deeply psychological. When a surgeon first mentioned "permanent" in a virtual consultation, the shock was profound. The patient’s internal dialogue reflected the societal stigma surrounding ostomies:
- Will it leak? Will it smell?
- What about intimacy and personal attraction?
- Will my contamination OCD spiral out of control?
Perhaps the most haunting question was the one of self-doubt: What if it doesn’t even help? This "self-gaslighting"—the internalized belief that one’s suffering is not "bad enough" to warrant radical intervention—is a common feature for those with rare, invisible chronic illnesses. Yet, comparing the potential for a new life to the reality of her current, restricted existence provided the clarity she needed to move forward.
Post-Operative Realities: The "New Normal"
The recovery process was anything but textbook. For a patient with EDS, healing is rarely linear, and the 10-hour colectomy was followed by a recovery period that required constant patient advocacy within the hospital setting. However, the result was transformative. The bloating, the chronic pain, and the feeling of heaviness that had plagued her for decades dissipated almost immediately upon the stoma becoming functional.
Life on the "other side" of the surgery has not been without its hurdles. Leaks happen, skin irritation is a reality, and there is a necessary period of grieving for the body one used to have. Yet, the outcome has been a profound reclamation of agency. Goectau has transformed her experience into a source of support for others, founding a small business creating custom ostomy bag covers and using her platform, @distaaybled, to document the unfiltered reality of living with a stoma.
Global Implications and Advocacy
The impact of this journey extends beyond the individual. Goectau’s advocacy has taken her to Kenya with Campaign 52, where she provides education and resources for women’s hospitals. Her work highlights a critical gap in global healthcare: the lack of accessible information and support for patients with non-standard GI conditions.
The implications for medical providers are clear:
- Listen to the Patient: When a patient with EDS reports chronic, treatment-resistant GI distress, it is not "all in their head."
- Look for Structural Causes: If standard interventions fail, investigate the structural and "rare" possibilities, such as visceral organ displacement or autonomic dysfunction.
- Validate the Struggle: Invisible, non-measurable symptoms are just as debilitating as those that show up on a standard scan.
Conclusion: A Livable Life
For those newly facing the prospect of an ostomy, the message is one of cautious hope. Grief and fear are valid, normal responses to such a significant transition. However, as Goectau’s experience demonstrates, there is a version of life after an ostomy that is not only livable but vibrant.
By centering the voices of those with lived experience, the medical community can move toward a more compassionate and effective approach to managing the complex, intersectional health challenges faced by the EDS community. The stoma-versary is more than a medical milestone; it is a testament to the fact that when the standard path fails, the right intervention—no matter how unconventional—can indeed save a life.
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, visceroptosis, or ostomies. Discussion of diagnostic testing, surgical interventions, and treatment outcomes is provided for educational purposes only and should not be interpreted as medical advice. Readers should consult their healthcare team regarding their individual circumstances.