





For decades, the gold standard for evaluating the success of obstructive sleep apnea (OSA) treatment has been the Apnea-Hypopnea Index (AHI). Clinicians have long celebrated the normalization of AHI as the primary metric for effective management. However, a growing body of clinical evidence—and the lived experiences of thousands of patients—suggests that treating the airway is not always synonymous with restoring the patient.
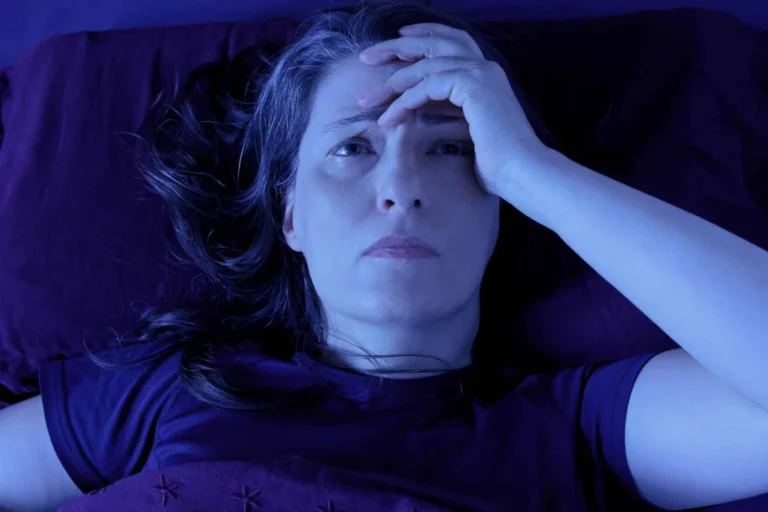
Even when OSA is effectively managed through CPAP therapy, oral appliances, or surgical intervention, a significant cohort of patients continues to struggle with excessive daytime sleepiness (EDS). This residual sleepiness is not merely a minor inconvenience; it is a profound clinical burden that erodes cognitive function, destabilizes personal relationships, hinders professional productivity, and diminishes overall quality of life.
To address this critical gap in sleep medicine, a landmark live webinar event is scheduled for Friday, May 29, 2026, at 9 AM ET/6 AM PT. This session, featuring renowned sleep experts Edward Mezerhane, MD, and Laura Bogan Herpel, MD, aims to shift the clinical paradigm away from simple AHI metrics toward a more holistic, functional approach to patient care in 2026 and beyond.
The Clinical Landscape: Why AHI Isn’t Enough
The Limitations of Traditional Metrics
The AHI was designed as a tool to quantify the severity of breathing disruptions during sleep. While it remains indispensable for diagnosing OSA, it fails to capture the complex, multifactorial nature of sleep architecture and its subsequent impact on wakefulness.
In many clinical settings, a patient who achieves an AHI of less than five events per hour is often considered "treated." Yet, these same patients frequently report "brain fog," microsleeps, and an inability to maintain alertness throughout the workday. This discrepancy highlights a critical flaw in current sleep medicine protocols: the assumption that anatomical patency equates to physiological recovery.
The Impact of Residual EDS
Residual EDS is a pervasive issue that ripples through every facet of a patient’s existence. In the workplace, it manifests as decreased executive function, slower reaction times, and diminished creativity. In social and familial settings, the irritability and lack of energy associated with chronic sleepiness can strain relationships and lead to social withdrawal. Perhaps most concerning is the risk to public safety; individuals with residual EDS are at a significantly higher risk for motor vehicle accidents and workplace injuries.
Chronology of a Shifting Paradigm
The evolution of sleep medicine has undergone several distinct phases, each moving closer to the patient-centered model that will be discussed in the upcoming May 2026 webinar.
- 1980s–1990s: The Anatomical Era: The focus was almost exclusively on the mechanical obstruction of the airway. Success was measured solely by the reduction of apnea events.
- 2000s–2010s: The Adherence Era: As CPAP technology improved, the industry shifted its focus to patient compliance. The conversation centered on mask fit, pressure settings, and the number of hours of nightly use.
- 2020s: The Functional Era: The current decade marks a pivotal shift. Clinicians are now recognizing that adherence does not guarantee alertness. We are moving into an era where "Real-World Functional Outcomes" and "Patient-Reported Outcomes" (PROs) are becoming the true north of sleep therapy.
This progression sets the stage for the May 29 webinar, which aims to formalize these emerging standards for the 2026 clinical landscape.
Supporting Data and the "Residual Burden"
Emerging research suggests that between 10% and 30% of patients who are adherent to their CPAP therapy continue to report significant daytime sleepiness. This data point is startling because it implies that for nearly a third of our patients, the standard of care is insufficient.
Cognitive and Physiological Correlates
Data from recent longitudinal studies indicate that residual EDS is often linked to:
- Sleep Fragmentation: Even if the airway is open, micro-arousals (often missed by standard scoring) can prevent the patient from achieving restorative REM and deep sleep stages.
- Comorbidities: Many OSA patients suffer from secondary conditions, such as periodic limb movement disorder (PLMD), depression, or metabolic syndrome, which may be masked by the primary OSA diagnosis.
- Circadian Dysrhythmia: Chronic sleep disruption can recalibrate a patient’s internal clock, meaning that even with a clear airway, their wake-sleep cycles remain misaligned.
The upcoming webinar will dissect these data points, providing attendees with the evidence required to advocate for more comprehensive diagnostic testing beyond the standard polysomnography.
Expert Perspectives: The Webinar Presenters
The May 29 event features two of the most respected voices in the field of sleep medicine. Their combined expertise ensures a balanced discussion that bridges the gap between theoretical research and bedside practice.
Dr. Edward Mezerhane, MD, FAASM, FACP, DABOM, CPI
As a Fellow of the American Academy of Sleep Medicine and a board-certified specialist in obesity medicine, Dr. Mezerhane brings a nuanced perspective to the discussion. His work emphasizes the intersection of metabolic health and sleep disorders. By viewing the patient through a broader lens—considering weight, diet, and hormonal balance—Dr. Mezerhane advocates for a multi-modal approach to treating residual sleepiness.
Dr. Laura Bogan Herpel, MD, FCCP
A Fellow of the American College of Chest Physicians, Dr. Herpel brings deep clinical expertise in respiratory medicine. Her focus is on the patient experience and the practical implementation of clinical strategies. She is a staunch proponent of utilizing Patient-Reported Outcome Measures (PROMs) to ensure that the patient’s subjective feeling of alertness is given as much weight as objective sensor data.
Implications for Clinical Practice in 2026
The implications of this shift are profound for sleep technologists, physicians, and primary care providers alike.
Moving Beyond AHI in the Clinic
What does "management" look like in 2026? According to the webinar presenters, it involves:
- Enhanced Assessment Tools: Moving beyond the Epworth Sleepiness Scale (ESS) to more sensitive metrics like the Functional Outcomes of Sleep Questionnaire (FOSQ).
- Targeted Pharmacotherapy: When anatomical treatment is maximized, physicians are increasingly looking at adjunctive therapies to target wakefulness-promoting pathways.
- Lifestyle Interventions: Addressing the inflammatory nature of sleep-disordered breathing through diet, exercise, and metabolic management.
The Role of Technology
The webinar will also touch upon the emerging technologies that allow for more granular monitoring of sleep, such as home-based sleep apnea testing (HSAT) with advanced signal processing and wearable devices that provide long-term data on sleep architecture rather than just nightly apnea counts.
Webinar Details and Registration
For those looking to earn Continuing Sleep Technology Education (CSTE) credits, this event is a vital opportunity. The Board of Registered Polysomnographic Technologists (BRPT) has designated this live webinar for a maximum of 1.0 CSTE credits.
Event Details:
- Date: Friday, May 29, 2026
- Time: 9 AM ET / 6 AM PT
- Format: Live presentation followed by an interactive Q&A session.
Registration Instructions:
Attendance is highly encouraged for sleep technologists, sleep physicians, respiratory therapists, and allied health professionals. Even if you cannot attend the live session, it is strongly recommended that you register today. All registrants will receive an email containing the recording of the webinar, ensuring that no one misses out on these critical insights.
To register for this event, please visit the official Sleep Review webinar portal.
Conclusion: A New Standard of Care
The medical community is at a turning point. For too long, the success of OSA treatment has been defined by the absence of disease (the absence of apneas) rather than the presence of health (the presence of alertness). By focusing on residual daytime sleepiness, we are acknowledging that our patients deserve more than just a "treated" diagnosis—they deserve a return to a vibrant, productive, and safe quality of life.
We invite you to join Dr. Mezerhane and Dr. Herpel on May 29, 2026, to be part of this essential conversation. Together, we can redefine the success of sleep medicine for the next generation of patients.
For those who wish to catch up on the foundational concepts, parts 1 and 2 of our excessive daytime sleepiness webinar series are currently available on demand. Part 1 can be found here, and Part 2 is accessible via our resource center.