For decades, the “lipid panel”—a staple of the annual physical—has been the primary compass by which physicians navigate the cardiovascular health of their patients. Millions of Americans have become accustomed to the ritual of fasting, drawing blood, and waiting for the results of their LDL (“bad”) cholesterol levels. However, a groundbreaking study from Northwestern Medicine suggests that our current navigational tools may be fundamentally flawed.
New research published in JAMA indicates that shifting our clinical focus from LDL cholesterol to apolipoprotein B (apoB) could revolutionize cardiovascular prevention. By identifying patients who truly require aggressive medical intervention, this shift promises to prevent a significant number of heart attacks and strokes across the United States.
The Science of Risk: Why LDL Isn’t the Whole Story
To understand the paradigm shift proposed by the researchers at Northwestern University Feinberg School of Medicine, one must first understand how heart disease manifests at a microscopic level. Cardiovascular disease remains the leading cause of mortality in the United States, placing an immense burden on both the public health infrastructure and the national economy.
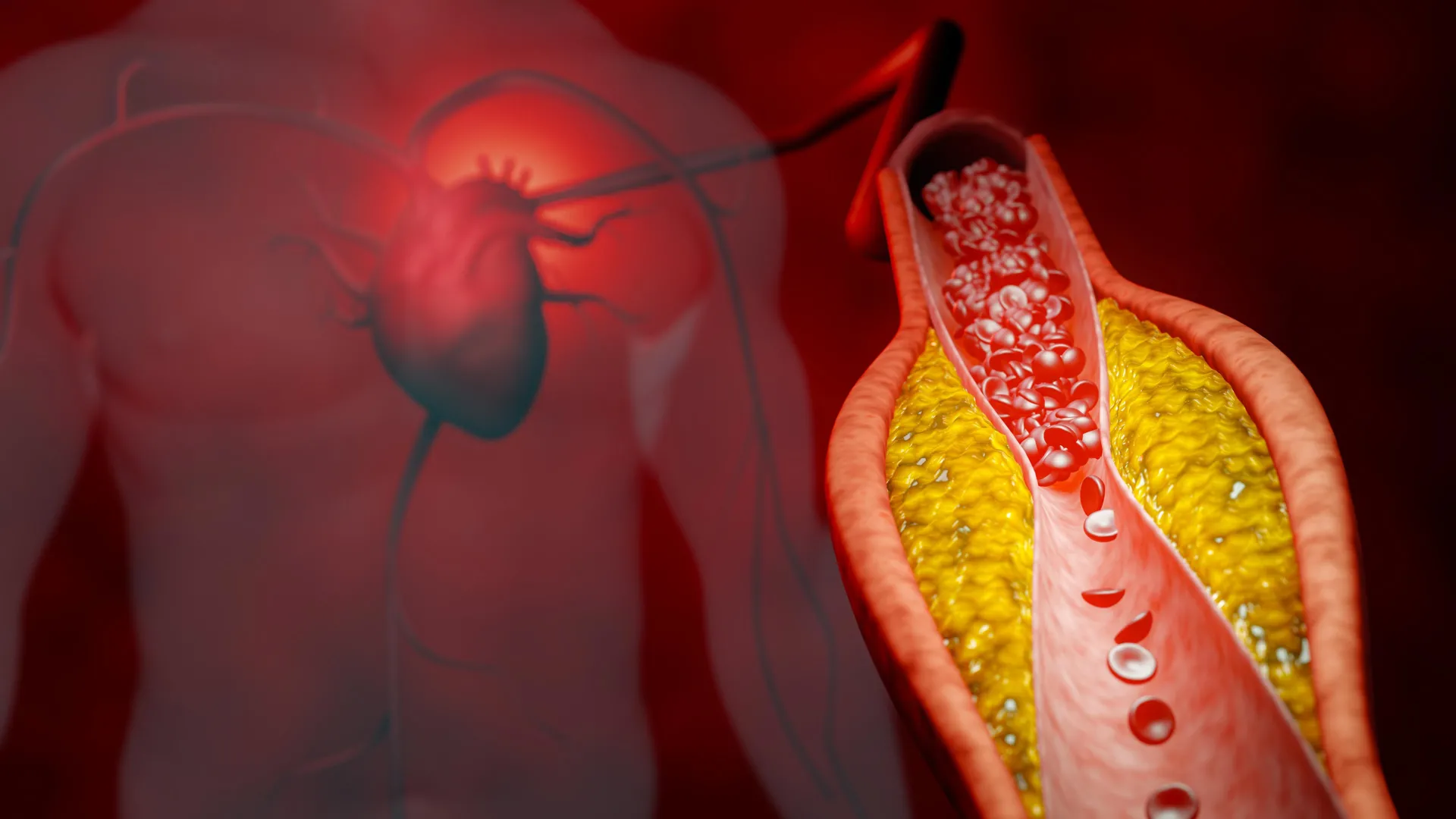
The process of atherosclerosis—the hardening and narrowing of the arteries—is driven by tiny, cholesterol-carrying particles circulating in the bloodstream. Over time, these particles can become trapped within the delicate endothelial lining of artery walls. Once lodged, they accumulate, forming plaques that restrict blood flow and set the stage for catastrophic events like heart attacks and strokes.
For years, clinical guidelines have relied on LDL (low-density lipoprotein) and non-HDL cholesterol as proxies for this risk. While these metrics provide valuable data, they are inherently limited. They measure the mass of cholesterol within these particles, but they do not account for the number of particles present.
“We found that apoB testing to intensify cholesterol-lowering medication would prevent more heart attacks and strokes than current practice,” explains lead author Ciaran Kohli-Lynch, assistant professor of preventive medicine at Northwestern. “Research strongly shows that apoB is better at identifying who is at risk because it counts the total number of harmful particles in the blood.”
In essence, while LDL tells a physician how much cholesterol is present, apoB reveals how many "delivery vehicles" are available to deposit that cholesterol into the arterial wall. Because each particle carries a single apoB molecule, measuring apoB serves as a direct, accurate census of the atherogenic particles threatening a patient’s health.
Chronology of a Clinical Evaluation
The study, titled "Cost-Effectiveness of ApoB, Non-HDL-C, and LDL-C Goals for Primary Prevention Lipid-Lowering Therapy," was not a mere observation of current trends; it was a rigorous simulation designed to test the long-term clinical and economic utility of these different diagnostic strategies.
The Modeling Framework
To determine if the extra cost and inconvenience of an apoB test were justified, the research team—which included Dr. John Wilkins and Dr. Samuel Luebbe—constructed a sophisticated computer simulation. The model represented a cohort of 250,000 U.S. adults who were eligible for statin therapy but had not yet developed clinical cardiovascular disease.
Comparing Strategies
The researchers evaluated three distinct clinical approaches:
- The LDL-C Approach: Using traditional LDL cholesterol thresholds to determine the necessity of statin therapy.
- The Non-HDL-C Approach: Using non-HDL cholesterol as the target for therapy.
- The ApoB Approach: Using the apoB count as the primary biomarker for guiding treatment intensity.
In each scenario, the researchers simulated a lifelong journey for these patients. If a patient failed to meet their specific target under their assigned strategy, the model "stepped up" their treatment—first by prescribing more potent statins, and subsequently by adding non-statin medications such as ezetimibe.
Measuring Success
The study tracked several key outcomes over the simulated lifetimes of the participants:
- Incidence of heart attacks and strokes.
- Overall life expectancy.
- Quality-adjusted life years (QALYs).
- Total healthcare spending and cost-effectiveness ratios.
The results were unequivocal: the apoB-guided strategy consistently outperformed both the LDL and non-HDL approaches. By targeting the number of harmful particles rather than their mass, clinicians could more precisely tailor therapy, leading to better cardiovascular outcomes at a cost that the researchers determined represents high value for the U.S. healthcare system.
Supporting Data: The Case for Cost-Effectiveness
One of the most persistent arguments against the universal adoption of apoB testing has been the logistical hurdle. Unlike the standard lipid panel, which is included in most routine checkups, measuring apoB often requires an additional blood draw and, in some cases, represents a higher upfront cost.
However, Dr. Kohli-Lynch’s research addresses this head-on. This is the first comprehensive analysis to demonstrate that the societal savings gained from preventing heart attacks and strokes far outweigh the marginal costs of additional testing.
“Our study asked: Is it worth spending extra money to use apoB instead of LDL to guide treatment intensification?” says Kohli-Lynch. The data suggest that the answer is a resounding yes. By avoiding the downstream costs of emergency room visits, hospitalizations, cardiac procedures, and chronic management of stroke survivors, the healthcare system achieves a net benefit. The simulation highlights that while the diagnostic phase may require more investment, the long-term clinical gains create a "good value" proposition for payers and patients alike.
Official Responses and Clinical Implications
The timing of this research is critical. Earlier this year, the American Heart Association and a coalition of ten other major medical organizations released updated clinical guidelines. These guidelines advocate for the initiation of cholesterol-lowering therapy at younger ages for a broader segment of the population.
As more Americans are identified as candidates for statin therapy earlier in life, the necessity for precision medicine becomes paramount. Over-treating healthy individuals leads to unnecessary side effects, while under-treating those at high risk leads to preventable mortality.
A New Era for Primary Prevention
The implications for primary care are profound. If adopted into routine practice, the apoB test could become the gold standard for "precision prevention." It allows physicians to have a more nuanced conversation with patients who may have "normal" LDL levels but still possess a high count of atherogenic particles—a phenomenon often referred to as "residual risk."
Despite the evidence, the transition will not be instantaneous. "One reason [apoB is not commonly used] is that measuring apoB generally requires an additional blood test beyond the standard cholesterol panel, increasing both cost and inconvenience,” notes Kohli-Lynch. The medical community must now weigh these logistical challenges against the clear, data-driven benefits of superior risk stratification.
Future Outlook: Translating Research into Practice
The path from a JAMA publication to a standard of care is rarely a straight line. For this study to impact the lives of millions, several steps must occur:
- Clinical Adoption: Physicians must become comfortable interpreting apoB levels in the context of other cardiovascular risk factors.
- Laboratory Standardization: As demand for apoB testing increases, diagnostic labs must ensure that their testing protocols are consistent, accessible, and affordable.
- Insurance Coverage: Payers must recognize the cost-effectiveness data provided by this study and adjust their coverage policies to include apoB as a reimbursable screening tool for those at risk.
As we look to the future, the work of Dr. Kohli-Lynch and his team provides a clear mandate. In an era where heart disease remains the leading cause of death, we can no longer afford to rely on proxies that tell only half the story. By moving toward a more accurate, particle-based metric, the medical community has the opportunity to shift the narrative from managing the aftermath of heart disease to proactively preventing its onset.
The study, supported by the American Heart Association Career Development Award, serves as a wake-up call for the medical community. While the lipid panel has served us well for decades, the evolution of cardiovascular science demands an evolution in our diagnostic tools. Precision in testing leads to precision in treatment—and for millions of Americans, that is the difference between a life of health and a life interrupted by cardiovascular crisis.