




Main Facts: The Challenge of the Invisible Illness
Bipolar disorder remains one of the most misunderstood mental health conditions, largely because its most debilitating symptoms occur within the internal architecture of the brain, invisible to the naked eye. Unlike physical ailments that present with clear clinical markers—a cast for a broken bone or a rash for an allergy—bipolar disorder manifests through fluctuations in mood, energy, and cognition that can easily be misinterpreted as personality flaws or simple "moodiness."
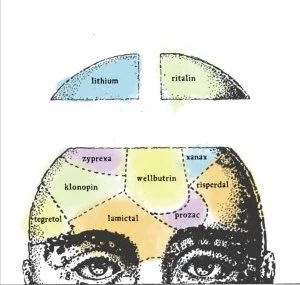
According to mental health expert and bestselling author Julie A. Fast, the difficulty in explaining the condition often stems from this lack of visible evidence. "It would be much easier for people to understand the condition if our brains bulged out of the sides of our heads when we became sick," Fast notes. Without such obvious indicators, those living with the disorder often face a "communication chasm" where their internal reality is at odds with their external appearance.
To bridge this gap, advocates suggest a shift away from clinical jargon toward "scripts"—memorized, simple patterns of speech designed to explain complex neurological states in plain language. The goal is to move the conversation from judgment to management, ensuring that family and friends understand that bipolar disorder is a medical condition requiring a specific treatment infrastructure, much like diabetes or cardiovascular disease.
Chronology: From "Manic Depression" to Modern Management
The history of communicating bipolar disorder has undergone a significant evolution over the last several decades. Historically, the condition was referred to as "manic depression," a term that carried heavy social stigma and often focused exclusively on the extreme poles of the illness.
In the early 2000s, the shift toward the term "bipolar disorder" aimed to reflect the clinical reality of the condition as a spectrum of mood dysregulation. Julie A. Fast, a pioneer in the field of bipolar management, began publishing her findings in 2004 with the release of Take Charge of Bipolar Disorder. Her work marked a turning point in how patients were taught to interact with their support systems.
Over the past twenty years, the "Fast Talk" methodology has evolved from basic symptom tracking to the implementation of sophisticated "management plans." This chronological shift reflects a broader movement in psychiatry: moving the patient from a passive recipient of care to an active manager of their own stability. By 2010, the concept of "scripts" became a staple in the coaching of patients, providing them with the linguistic tools to navigate crises before they escalated into relationship-ending conflicts.
The integration of these strategies into popular culture—such as Fast’s consultancy for the character Carrie Mathison on the TV show Homeland—further chronicled the transition of bipolar disorder from a "hidden shame" to a visible, manageable, albeit difficult, medical reality.
Supporting Data: The Impact of Miscommunication
The necessity for clear communication is backed by sobering statistics regarding the social and personal toll of bipolar disorder. Research indicates that individuals with bipolar disorder often face higher rates of divorce, job loss, and social isolation compared to the general population.
- Relationship Stability: Studies show that nearly 90% of marriages involving an individual with bipolar disorder may face significant distress, with many ending in divorce. This is often attributed to the "unpredictability" of manic or depressive episodes.
- The Neurobiology of Perception: Mania and depression are not just "feelings"; they are physiological states. During a manic episode, the prefrontal cortex—the area of the brain responsible for impulse control and logical reasoning—can become underactive, while the amygdala, which processes emotions, becomes hyperactive. This explains why a person in a manic state may literally be unable to "just calm down."
- The Power of Routine: Data suggests that Social Rhythm Therapy (SRT), which emphasizes a strict schedule for sleeping, eating, and exercise, is one of the most effective non-pharmacological interventions for bipolar disorder. This supports the need for "scripts" that explain to friends why a change in plans (which disrupts this rhythm) can be medically detrimental.
By using simple terms to explain these data points—such as comparing a manic brain to a car with a stuck accelerator—patients can help their loved ones visualize the physiological reality of the disorder.
Official Responses: Expert Strategies for Dialogue
Mental health professionals and researchers emphasize that the "how" of communication is just as important as the "what." The consensus among experts like Fast is that effective communication must be proactive rather than reactive.
The Role of "Scripts"
Experts advocate for the use of pre-planned scripts. These are not intended to be robotic, but rather to provide a cognitive anchor during times of stress. When a person is depressed or manic, their ability to find the right words diminishes. A script acts as a safety net.
One such script addresses the need for a set schedule:
"Scheduling is vital to my stability. If plans change at the last minute, it can trigger a depressive dip. I know this can be frustrating for you, and I appreciate your flexibility, but I need you to know why I value punctuality so highly."
Distinguishing Moodiness from Episodes
A critical component of the expert-led approach is teaching family members the difference between "normal moodiness" and a "bipolar episode."
- Moodiness is usually a reaction to an external trigger (a bad day at work) and is consistent with a person’s personality.
- Bipolar Episodes are often out of proportion to triggers or occur with no trigger at all. They are episodic, meaning they have a distinct beginning and end, and they can fundamentally alter behavior in ways that are inconsistent with the person’s true character.
Accountability and Treatment
A key official stance from mental health advocates is that an explanation is not a justification. "Explaining bipolar disorder does not mean justifying hurtful behavior," Fast asserts. Experts agree that the most successful communication occurs when the patient takes full responsibility for their treatment plan. This "official response" to the illness involves a two-way contract: the patient works toward stability, and the loved one provides a supportive environment based on informed understanding.
Implications: Communication as Preventive Medicine
The long-term implications of mastering these communication strategies are profound. When bipolar disorder is framed correctly—as a chronic but manageable brain-based illness—the dynamic of the relationship shifts from "caregiver vs. patient" to "partners against the disorder."
Prevention of Relationship Attrition
The primary implication of using scripts and simple language is the preservation of the support network. Bipolar disorder can be "exhausting" for friends and family. Clear communication reduces the "confusion-anger-distrust" cycle that often leads to the end of friendships and domestic partnerships. When a loved one understands the "why" behind a behavior (e.g., "His brain is currently sending distorted messages"), they are less likely to take the symptoms personally.
Destigmatization Through Education
By comparing bipolar disorder to diabetes, patients contribute to a broader societal shift. This analogy implies that while the patient didn’t choose the illness, they have a daily responsibility to manage it through medication, diet, and lifestyle choices. This framing reduces the "moral failing" stigma and encourages more people to seek help.
Improved Clinical Outcomes
There is a direct correlation between social support and clinical stability. Patients who can successfully communicate their needs to their inner circle are more likely to adhere to their medication schedules and maintain the regular sleep patterns necessary for health. In this sense, the "scripts" described by Fast are more than just social tools—they are a form of preventive medicine that keeps the patient out of the hospital and integrated into their community.
Ultimately, the goal of enriching the dialogue around bipolar disorder is to ensure that while the symptoms may remain invisible, the person living with them feels seen, heard, and supported. As Fast concludes, when patients do everything in their power to explain the illness, they make it easier for others to love them—a fundamental requirement for long-term recovery.