










Introduction: The Unraveling of the Medical Narrative
For decades, the field of psychiatry has sought to anchor its professional authority in the bedrock of biological science. The prevailing narrative suggested that mental health conditions are "diseases like any other," grounded in objective, value-free biological facts that would eventually be uncovered through neuroscience and genetics. However, a significant tremor has recently shaken the foundations of this clinical edifice.
In a landmark essay titled "The Ground Beneath the Clinic," published in Psychiatry Margins, Dr. Awais Aftab—an influential psychiatrist and philosopher known for his deep dives into the conceptual foundations of the field—has made a startling admission. He concedes that the long-standing project of defining psychiatric authority through the lens of objective, value-free disorder concepts has failed.
This is not a peripheral critique from an outsider; it is a profound concession from within the heart of the profession. Aftab’s admission signals a turning point in how we understand human suffering, shifting the conversation from "what is wrong with your brain" to a much more complex, value-laden inquiry into the nature of the human condition.
I. Main Facts: The Admission of a Failed Project
The core of the current debate centers on the "legitimating narrative" of psychiatry. Since the mid-20th century, the profession has relied on the "Medical Model" to justify its power to diagnose, medicate, and sometimes institutionalize individuals. This model presumes that mental disorders are discrete biological entities waiting to be discovered by science.
The Aftab Concession
Dr. Aftab’s essay explicitly states: "I take it for granted that the project of defining the authority of medicine and clinical disciplines in terms of disorder concepts on the basis of objective, value-free facts has failed."
By "value-free facts," Aftab refers to the idea that a diagnosis like "Major Depressive Disorder" or "Schizophrenia" could be identified with the same biological certainty as a broken leg or a bacterial infection. The failure of this project means that psychiatry cannot claim to be a neutral observer of biological malfunctions. Instead, it must reckon with the fact that its diagnoses are inextricably tied to social norms, cultural expectations, and moral judgments.
The Death of the "Chemical Imbalance"
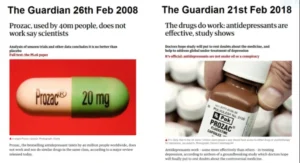
Aftab’s admission comes on the heels of a broader collapse of simplified biological narratives, most notably the "chemical imbalance" theory of depression. While many clinicians had moved away from this theory years ago, the public-facing side of psychiatry continued to use it as a shorthand for legitimacy. The recognition that these narratives are insufficient creates a "crisis of authority": if psychiatry isn’t just fixing broken brain chemistry, what exactly is it doing?
II. Chronology: The Rise and Fall of the Biological Imperative
To understand the weight of Aftab’s concession, one must look at the historical trajectory of psychiatric thought over the last century.
1950s–1970s: The Era of Ambiguity
Before the 1980s, psychiatry was dominated by psychoanalytic thought and vague "psychosocial" descriptions. Diagnoses were often unreliable; two different doctors might see the same patient and provide two different labels. This lack of reliability led to a crisis of confidence, as critics like Thomas Szasz argued that mental illness was a "myth" used for social control.
1980: The DSM-III Revolution
In response to these critiques, the American Psychiatric Association (APA) released the DSM-III, led by Dr. Robert Spitzer. This version of the Diagnostic and Statistical Manual of Mental Disorders attempted to make psychiatry "scientific" by focusing on observable symptoms rather than underlying psychological theories. This was the birth of the modern medical model in psychiatry—an attempt to standardize "disorders" as if they were biological diseases.
1990s: The "Decade of the Brain"
The 1990s saw an explosion of optimism. With the advent of functional MRI (fMRI) and the Human Genome Project, leaders in the field predicted that the "biological markers" for every major mental illness would be found within a decade. It was during this time that the pharmaceutical industry heavily marketed the "chemical imbalance" theory to the public.
2010s: The Failure of the Biological Hunt
By the mid-2010s, the optimism began to sour. Despite billions of dollars in research, no genetic test, blood test, or brain scan had been developed that could reliably diagnose a single mental disorder. In 2013, Dr. Thomas Insel, then-director of the National Institute of Mental Health (NIMH), famously criticized the DSM for its "lack of validity," stating that psychiatric diagnoses were based on clusters of symptoms rather than objective laboratory measures.
2024: The Ground Beneath the Clinic
Dr. Aftab’s recent essay represents the culmination of this historical arc. It is an acknowledgment that the "biological revolution" did not deliver the objective foundation it promised.
III. Supporting Data: The Evidence of Conceptual Instability
The admission that psychiatric authority cannot be grounded in value-free facts is supported by several decades of research data that highlight the limitations of the purely medical approach.
1. The Lack of Biomarkers
In physical medicine, a "biomarker" (like blood glucose for diabetes) is the gold standard for diagnosis. In psychiatry, after 50 years of intensive neuroimaging, there are still no clinical biomarkers. A 2022 meta-review of neuroimaging studies published in Nature concluded that most brain-wide association studies were too small and inconsistent to provide reliable markers for mental health conditions.
2. The Heterogeneity of Diagnoses
The data shows that two people diagnosed with the same disorder, such as Post-Traumatic Stress Disorder (PTSD), can share zero symptoms. With thousands of possible symptom combinations for a single diagnosis, the concept of a "discrete disorder" becomes statistically and clinically fragile.
3. The Placebo Gap
Large-scale meta-analyses of antidepressant efficacy have shown that while medications do help some individuals, the "placebo effect" accounts for a significant portion of the improvement. This suggests that the meaning and context of treatment are often as powerful as the chemical intervention, further undermining the idea of a purely biological fix.
4. Cultural Variation
Data from cross-cultural psychiatry shows that "disorders" manifest differently across the globe. For example, the experience of "depression" in Western cultures often focuses on internal emotional states (guilt, sadness), whereas in many Eastern cultures, it manifests as physical symptoms (fatigue, body aches). If disorders were "objective, value-free facts," they would not change so drastically based on cultural geography.
IV. Official Responses and the Spectrum of Opinion
The admission that psychiatry lacks a value-free foundation has triggered a range of responses from the medical community, advocacy groups, and philosophers of science.
The "Critical Psychiatry" Perspective
Groups like the Critical Psychiatry Network (CPN) have welcomed Aftab’s concessions. For these practitioners, the failure of the medical model is an opportunity to move toward a "social-material" model. They argue that mental distress is often a rational response to poverty, trauma, and social isolation, rather than a "disorder" inside the head.
The APA and the "Biopsychosocial" Defense
The American Psychiatric Association (APA) and other mainstream bodies have generally pivoted to the "biopsychosocial model." This model suggests that while we haven’t found the specific biological causes yet, biology still plays a role alongside psychological and social factors. However, critics argue this is often a "lip-service" model where the "bio" part still receives 90% of the funding and attention.
The Patient Advocacy Divide
Response among service users is deeply split:
- The "Validation" Group: Many patients find the biological narrative helpful. For them, a "brain disease" label reduces the stigma of being "weak" or "lazy." They fear that moving away from the medical model will result in a loss of insurance coverage and a return to blaming the individual for their suffering.
- The "Pathologized" Group: Other survivors of the psychiatric system argue that the medical model has "gaslit" them by ignoring the real-world causes of their distress (such as childhood abuse) and reducing their life experiences to "faulty wiring."
V. Implications: Who Gets to Define Human Suffering?
If Dr. Aftab is correct and the authority of psychiatry cannot be grounded in objective, value-free facts, the implications are seismic. This shift touches on ethics, law, and the very nature of clinical practice.
1. The Ethics of Involuntary Treatment
Currently, the legal system allows for the involuntary commitment of individuals "due to a mental disorder." If the concept of a "disorder" is not an objective fact but a value-laden social judgment, the ethical justification for stripping someone of their liberty becomes much more precarious. On what basis does a psychiatrist claim the authority to override a person’s autonomy if they cannot point to a biological lesion?
2. The Definition of "Normal"
Without an objective biological baseline, the definition of "normal" behavior becomes a matter of social consensus. This opens the door to "diagnostic creep," where an increasing number of human experiences—grief, shyness, childhood rambunctiousness—are medicalized. If there is no biological "line in the sand," who decides where "eccentricity" ends and "illness" begins?
3. Clinical Practice: From "Curing" to "Meaning-Making"
For clinicians, this paradigm shift suggests a move away from the "technician" model of psychiatry. If the goal is not simply to "fix" a biological mechanism, the psychiatrist’s role becomes one of a "hermeneutic guide"—someone who helps the patient find meaning in their suffering and navigate their social environment.
4. The Future of Research
The failure of the value-free project necessitates a new direction for research. Instead of searching for the "depression gene," future research may focus on the "ecology of the mind"—studying how environmental stressors, social structures, and personal narratives interact with human biology.
5. The "Authority" Gap
Perhaps the most pressing question is the one Aftab leaves us with: What follows from this admission?
If psychiatry loses its status as a "hard science," it must find a new way to justify its place in the medical hierarchy. Aftab suggests that psychiatric authority might instead be grounded in "clinical utility" and "human flourishing." In this view, psychiatry is not a science of "what is," but a practice of "what helps."
Conclusion: A More Humble Science
The concession by Awais Aftab marks the end of an era of psychiatric triumphalism. The dream of a purely biological, value-free psychiatry has proven to be a mirage. However, this does not mean that psychiatry is useless or that mental suffering isn’t real.
Rather, it suggests that psychiatry is a unique discipline that sits at the intersection of biology, philosophy, and social justice. By admitting that it cannot rely on objective facts alone, the field may finally be able to embrace a more honest and holistic approach to human suffering—one that acknowledges that the "ground beneath the clinic" is not made of neurons and synapses alone, but of the complex, messy, and deeply value-laden experience of being human.





