









For decades, the medical community has viewed the aging of human skin as an inevitable, irreversible decline. As the body enters its later years, the skin—our largest organ—thins, loses elasticity, and, perhaps most critically, loses its ability to knit itself back together after injury. From the slow closure of surgical incisions to the stubborn persistence of chronic wounds in diabetic patients, the limitations of geriatric tissue repair have remained a significant clinical hurdle.
However, a groundbreaking line of research is shifting the paradigm. Scientists are moving away from treating the symptoms of aging skin and are instead focusing on the underlying cellular "clutter" that prevents healing. A study published in Aging (Aging-US), conducted by a team at the Boston University Aram V. Chobanian and Edward Avedisian School of Medicine, suggests that a specific class of drugs—senolytics—could be the key to "resetting" the skin’s biological clock to facilitate rapid recovery.
The Problem with ‘Zombie Cells’
To understand the breakthrough, one must first understand the concept of cellular senescence. Throughout our lives, cells divide and multiply to keep our tissues healthy. Eventually, however, cells reach a limit. When a cell becomes damaged or stressed, it may enter a state of "senescence."
These senescent cells are often colloquially dubbed "zombie cells." They are no longer functional; they have ceased their normal role in maintaining tissue integrity, yet they refuse to die. Instead, they linger, secreting a cocktail of inflammatory chemicals and signaling molecules known as the Senescence-Associated Secretory Phenotype (SASP).
In younger individuals, the immune system acts as a cleanup crew, identifying and disposing of these senescent cells before they can cause trouble. As we age, however, this immune surveillance falters. Senescent cells accumulate, creating a toxic microenvironment that stifles the regeneration of healthy tissue. For an older adult, this means that even a minor cut or a routine surgical incision faces a biological landscape hostile to repair, leading to the delayed healing and high complication rates frequently observed in clinical practice.
The Chronology of Discovery: From Bench to Bedside
The investigation into using the drug ABT-263—a potent senolytic—as a topical treatment for skin repair represents a significant evolution in regenerative medicine.
The Initial Breakthrough (2024)
The Boston University study, led by researchers including Maria Shvedova and Daniel S. Roh, hypothesized that if these senescent cells were the primary bottleneck in aging skin, then selectively eliminating them should unleash the body’s latent healing potential.
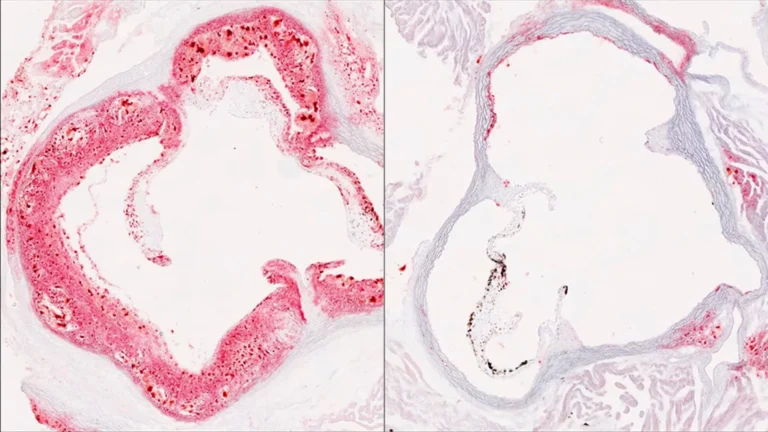
In their experiment, the team applied ABT-263 topically to aged mice for five days. The results were stark: the treatment significantly reduced the burden of senescent cells in the skin. When the researchers then introduced controlled wounds, the treated mice exhibited a profound healing advantage. By day 24, an impressive 80% of the treated cohort had achieved full wound closure, compared to only 56% of the untreated control group.
Expanding the Scope (2025–2026)
Following the publication of the BU findings, the field gained momentum. In 2025, a comprehensive review in Ageing Research Reviews solidified the consensus that cellular senescence is not merely a byproduct of aging but a driver of chronic skin pathology.
The momentum accelerated in 2026 with a study that addressed one of the most difficult challenges in modern medicine: diabetic wound healing. Diabetic patients frequently suffer from chronic, non-healing ulcers due to poor circulation and persistent inflammation. By developing a specialized wound dressing infused with ABT-263, researchers were able to demonstrate improved healing in diabetic models without the systemic toxicity that often plagues oral medications. This marked a shift from systemic senolytic therapy to localized, "precision" applications.
Supporting Data: The Paradox of Inflammation
One of the most intriguing aspects of the BU study was the observation of an acute, short-lived inflammatory response immediately following the application of ABT-263.
Historically, inflammation has been painted as the villain in the wound-healing process. Chronic inflammation is known to cause tissue destruction. However, the study revealed that a controlled, localized "burst" of inflammation served as a catalyst for recovery. By clearing the senescent cells, the treatment appeared to "wake up" dormant signaling pathways.
Gene expression analysis showed a significant upregulation in pathways related to:
- Collagen Synthesis: The primary structural protein required to rebuild skin.
- Angiogenesis: The growth of new blood vessels to supply oxygen to the wound bed.
- Tissue Remodeling: The process of organizing new cells into functional, durable tissue.
This suggests that aging skin is not necessarily incapable of healing, but rather "confused" or "blocked." By removing the cellular debris, the drug restored the skin’s ability to initiate these critical repair sequences.
Official Perspectives and Scientific Caution
While the data from mice models is compelling, the scientific community remains cautiously optimistic. Dr. Daniel S. Roh and his colleagues emphasize that while their work underscores the potential for preoperative care, the transition to human clinical trials requires rigorous vetting.
"Our study underscores the potential of topical senolytic treatments to enhance wound healing in aging skin, presenting a potentially promising strategy for preoperative care," the team noted in their reporting.
However, the field is also grappling with the nuance of senescent cells. A 2024 review in Frontiers in Immunology provided a necessary counterweight to the "all-out war" on zombie cells. The authors pointed out that senescence is not universally harmful; in the very early stages of a fresh wound, a controlled amount of senescence can actually help coordinate the immune response and prevent excessive bleeding.
The challenge for future pharmacology is precision. Scientists are not just looking for a way to kill senescent cells; they are looking for the "goldilocks" zone—removing the chronic, harmful accumulation that prevents healing, without disrupting the body’s natural, immediate response to injury.
Clinical Implications: A New Standard of Care?
If these findings translate successfully to humans, the implications for geriatric medicine are vast. Currently, the "standard of care" for poor wound healing is often reactive—using advanced bandages, negative pressure therapy, or hyperbaric oxygen chambers only after a wound has failed to close.
A topical senolytic cream could change the strategy to a proactive one. Consider the following potential clinical applications:
1. Preoperative Priming
Surgeons could prescribe a short, topical course of senolytics to patients in the weeks leading up to elective surgery (such as hip replacements or skin cancer excisions). By "priming" the skin, surgeons could significantly reduce the risk of surgical site infections and dehiscence (the splitting open of a wound), which are common complications in older patients.
2. Treating Chronic Diabetic Ulcers
Diabetic foot ulcers are a leading cause of amputation. The 2026 research into localized dressings suggests that we may be on the verge of treating these wounds at the cellular level, turning a chronic, life-threatening condition into a manageable, temporary injury.
3. Geriatric Dermatology
Beyond wounds, the reduction of senescence could improve the overall resilience of elderly skin. This might help protect the skin from environmental stressors, improve skin barrier function, and potentially reduce the incidence of age-related skin fragility.
The Path Forward: What Remains to be Done?
Despite the enthusiasm, we are still in the early stages. The jump from murine models to human physiology is the most significant hurdle in pharmaceutical research. Humans have more complex immune systems, different skin thicknesses, and longer lifespans, all of which influence how senescent cells behave.
Key questions that remain unanswered include:
- Dosing and Frequency: What is the optimal concentration of a topical senolytic? How often should it be applied to ensure efficacy without damaging healthy, neighboring cells?
- Long-Term Safety: Could long-term use of senolytics have unintended consequences for skin health or pigment stability?
- Clinical Efficacy: Will the accelerated healing observed in mice hold up in the high-stress environment of human surgery?
The research conducted by the Boston University team and their contemporaries serves as a beacon for what is possible. By viewing aging not as a static state of decay but as a dynamic, cellular process that can be interrupted, science is finding ways to reclaim the body’s lost vitality. As the global population ages, the development of these therapies will move from the periphery of laboratory curiosity to the center of clinical necessity.
For the millions of seniors who face the prospect of slow recovery from injury or surgery, the "zombie cell" theory offers more than just academic interest—it offers the promise of a future where age is no longer a barrier to healing.