KINSHASA, Congo — A volatile health crisis is unfolding in the Democratic Republic of the Congo (DRC) as authorities grapple with an outbreak of the Bundibugyo strain of the Ebola virus—a rare and lethal variant for which there are currently no approved vaccines or targeted therapeutics. The outbreak, which has now claimed over 118 lives and infected more than 300 individuals, has prompted the World Health Organization (WHO) to declare a Public Health Emergency of International Concern.
The situation took an alarming turn this week when it was confirmed that an American doctor, identified as Dr. Peter Stafford, has contracted the virus. Dr. Stafford, who was actively treating patients at a hospital in Bunia, the capital of Ituri province, began exhibiting symptoms over the weekend. Following the diagnosis, a group of seven Americans—including the infected physician—have been evacuated and are being transported to Germany for specialized monitoring and care.
A Chronology of a Delayed Response
Public health experts and aid organizations are now raising critical questions regarding the speed of the government’s response. According to health records, the first fatality associated with this outbreak occurred on April 24 in Bunia. Following traditional burial practices, the body was transported to the Mongbwalu health zone—a densely populated mining region. Officials believe this movement of the deceased served as a catalyst, accelerating the virus’s transmission across provincial borders.
The timeline of the detection highlights the catastrophic consequences of diagnostic hurdles:
- April 24: The first suspected Ebola-related death occurs in Bunia.
- April 26: A second individual falls ill; samples are subsequently sent to the capital, Kinshasa, for laboratory analysis.
- May 5: The WHO is formally alerted to a cluster of approximately 50 deaths in the Mongbwalu zone, including four frontline healthcare workers.
- May 14: After weeks of uncertainty, the first official case of Ebola is confirmed.
- May 15: Laboratory analysis confirms the presence of the Bundibugyo strain, a rare variant distinct from the more common Zaire strain.
The initial delay was exacerbated by a "diagnostic blind spot." Because local health facilities were testing samples against the Zaire strain—the most frequent culprit in past Congolese outbreaks—the Bundibugyo cases initially returned false negatives. This diagnostic error effectively cost responders several weeks of critical containment time.
The Science of the Bundibugyo Strain
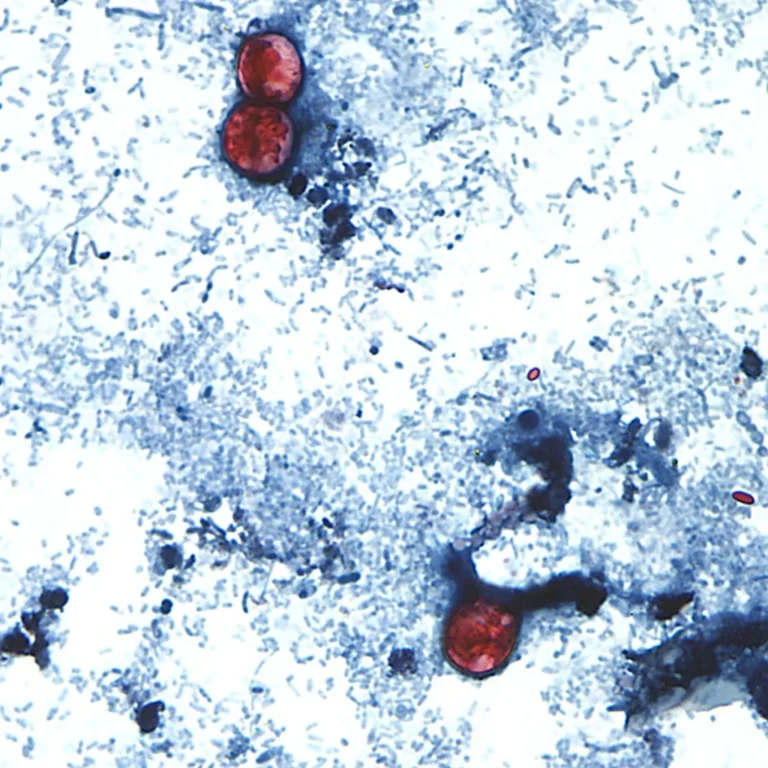
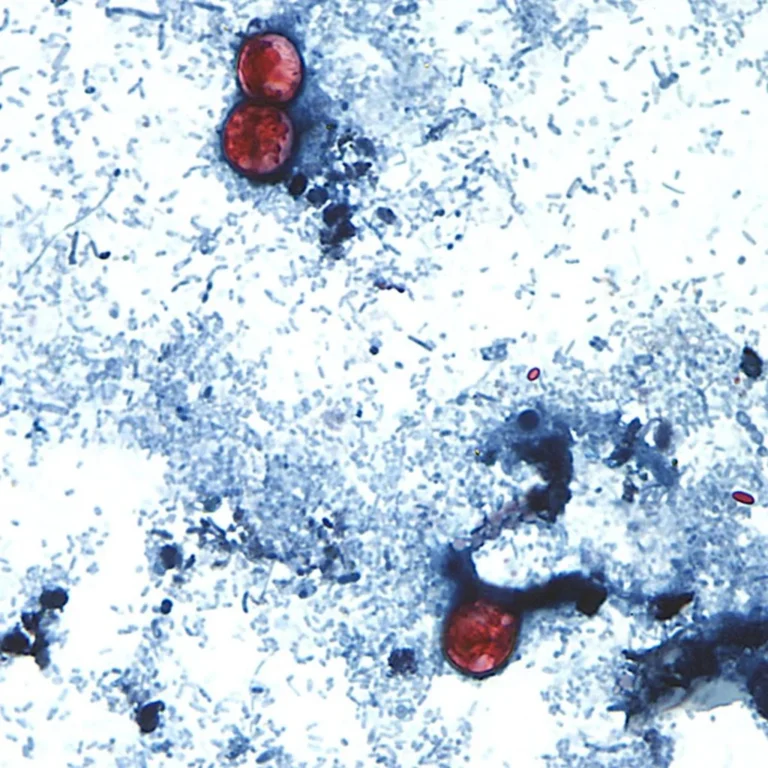
Ebola remains one of the world’s most feared pathogens, characterized by its high mortality rate and transmission via bodily fluids, including blood, vomit, and semen. While the Zaire strain is well-documented and currently managed by various medical countermeasures, the Bundibugyo variant is significantly less understood.
The Bundibugyo virus was first identified in the Bundibugyo district of Uganda during a 2007–2008 outbreak that resulted in 149 infections and 37 deaths. It reappeared in 2012 in Isiro, Congo, claiming 29 lives. Because it is so rare, clinical experience is limited, and the absence of established vaccines or dedicated therapeutics leaves medical teams in a state of high alert.
Dr. Gabriel Nsakala, a professor of public health with extensive experience in viral hemorrhagic fevers, noted that while Congo has built a robust infrastructure for managing Ebola, the nature of this specific variant complicates the clinical protocol. "We are essentially writing the playbook as we go," he stated. Dr. Jean Kaseya, the Africa CDC chief, echoed this sentiment, admitting he is in "panic mode" due to the current shortage of specialized medicines, though he noted that candidate treatments are being expedited to the region.
Official Responses and Geopolitical Tensions
The international community is now scrambling to provide support, but the response is being overshadowed by political finger-pointing and concerns over previous international policy decisions.
Matthew M. Kavanagh, director of the Georgetown University Center for Global Health Policy and Politics, offered a scathing critique of the current state of global preparedness. He argued that the erosion of funding for international health institutions has left the world vulnerable. "When you pull billions out of the WHO and dismantle frontline USAID programs, you gut the exact surveillance system meant to catch these viruses early," Kavanagh said. He characterized the current effort as a desperate attempt to "play catch-up against a very dangerous pathogen."
In response to the crisis, Congolese Health Minister Samuel Roger Kamba announced the establishment of three new specialized Ebola treatment centers. The WHO has deployed teams of epidemiologists and medical supplies, though the efficacy of these measures remains to be seen given the geographical challenges of the region.
The U.S. Centers for Disease Control and Prevention (CDC) has issued strict travel advisories, urging citizens to avoid contact with individuals displaying symptoms such as fever, muscle pain, and unexplained bleeding. Furthermore, the agency has implemented enhanced screening measures at ports of entry to identify potential cases arriving from the affected provinces.
Humanitarian and Regional Implications
The outbreak is occurring against a backdrop of long-standing instability in eastern Congo. Ituri and North Kivu provinces are home to over 273,000 internally displaced persons, many of whom live in crowded, unsanitary conditions that are ideal for the rapid spread of infectious diseases. The presence of armed rebel groups has further hindered humanitarian access, making it difficult for aid workers to conduct contact tracing or safe burials.
The humanitarian impact is profound. "No one really has a full understanding of how serious this crisis is," said a U.N. official based in Bunia. "We are asking staff to work from home and avoid physical contact, but we are terrified of having to halt operations entirely in a region that is almost completely dependent on our aid."
Regional neighbors are also taking defensive measures. On Sunday, Rwanda shuttered its land border with the DRC, allowing entry only to those with international flight tickets. This move has further isolated the affected regions, complicating the logistics of delivering aid and equipment.
The Path Forward
As the death toll climbs and the virus spreads to major hubs such as Goma and Butembo, the focus has shifted toward containment and the hope for emerging therapies. The evacuation of the American medical staff has highlighted the risks faced by aid workers, who remain the first line of defense in these remote, high-risk environments.
For now, the strategy remains centered on three pillars: rapid detection, strict isolation, and the implementation of ring vaccination protocols, provided that effective vaccines can be sourced for this specific variant. However, the success of these measures depends heavily on the cooperation of local populations, many of whom remain wary of government interventions due to the region’s history of conflict.
"The situation is quite worrying and is evolving pretty quickly," said Esther Sterk of Medecins Sans Frontieres. "But this is the reality of Ebola. It mimics other tropical diseases, it hides in the bush, and it thrives where healthcare systems are fragile. We have to be faster than the virus, or the consequences will be measured in thousands of lives."
As the world watches, the DRC finds itself at a crossroads. The combination of a rare, misunderstood variant, a delayed initial response, and a fragile humanitarian landscape presents a formidable challenge that will test the resolve and coordination of the international health community for months to come.