For the first time since 2018, the medical landscape regarding cardiovascular health has undergone a seismic shift. On March 28, 2026, the American College of Cardiology (ACC) and the American Heart Association (AHA) unveiled their highly anticipated updated clinical guidance on the screening and management of blood cholesterol. Presented at the ACC’s 75th Annual Scientific Session in New Orleans and published simultaneously in the Journal of the American College of Cardiology and Circulation, these recommendations represent a fundamental departure from the reactive medicine of the past, pushing toward a model of proactive, lifelong cardiovascular protection.
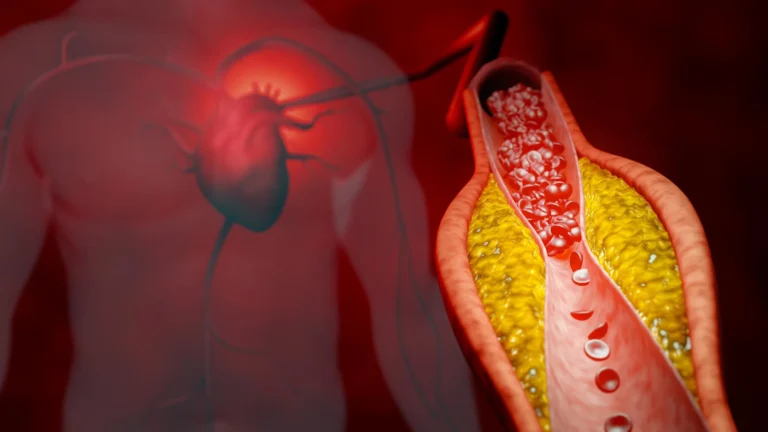
This comprehensive update arrives in tandem with a crucial supporting paper, "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026," published in the American Journal of Preventive Cardiology. Together, these documents provide a modernized framework for clinicians to combat the persistent threat of atherosclerosis—the silent, systemic narrowing of arteries that remains the leading cause of mortality worldwide.
A Chronology of Change: Moving Beyond the 2018 Framework
To understand the magnitude of these updates, one must look back at the trajectory of cardiovascular medicine over the last eight years. The 2018 guidelines were revolutionary in their time, solidifying the role of statins and identifying "risk enhancers" that helped clinicians look beyond traditional blood pressure and cholesterol numbers. However, the medical community has since accumulated a vast repository of data suggesting that the traditional approach—waiting until middle age to assess cardiovascular risk—was a missed opportunity.
The journey to the 2026 guidelines began with a rigorous multi-year synthesis of clinical trial data, including groundbreaking research like the VESALIUS-CV trial. By incorporating evidence from over 6.6 million patients—a massive leap from the 26,000 individuals represented in earlier models—the writing committee sought to create a more inclusive, accurate, and predictive set of standards. This update is not merely a revision; it is a recalibration of how we define "heart-healthy" across the human lifespan.
The Science of Risk: The PREVENT Calculator and Early Intervention
At the heart of the new guidance is a paradigm shift in how physicians calculate risk. The previous models were often limited to 10-year risk estimates for individuals aged 40 and older. The 2026 guidelines introduce the Predicting Risk of Cardiovascular Disease EVENTs (PREVENT) calculator, a robust tool that expands the horizon of risk prediction.
Expanding the Predictive Horizon
The PREVENT tool is designed for use starting at age 30, acknowledging that the biological processes leading to heart attack and stroke begin decades before symptoms emerge. Unlike its predecessors, which focused primarily on age, cholesterol, and blood pressure, the new calculator integrates vital indicators like kidney function and blood sugar levels. This multidimensional approach allows for a "30-year risk" assessment, providing younger adults with a clearer picture of their long-term health trajectory and the potential impact of early interventions.
Identifying Hidden Threats
The guidance places a renewed emphasis on "risk enhancers" that were previously overlooked. Clinicians are now urged to look deeper into a patient’s medical and genetic history. Factors such as a family history of premature atherosclerosis, systemic inflammatory conditions like rheumatoid arthritis, and complications during pregnancy—including preeclampsia and gestational diabetes—are now formally recognized as indicators that a patient may require more aggressive management.
The Core Strategy: LDL, Lipids, and Personalized Targets
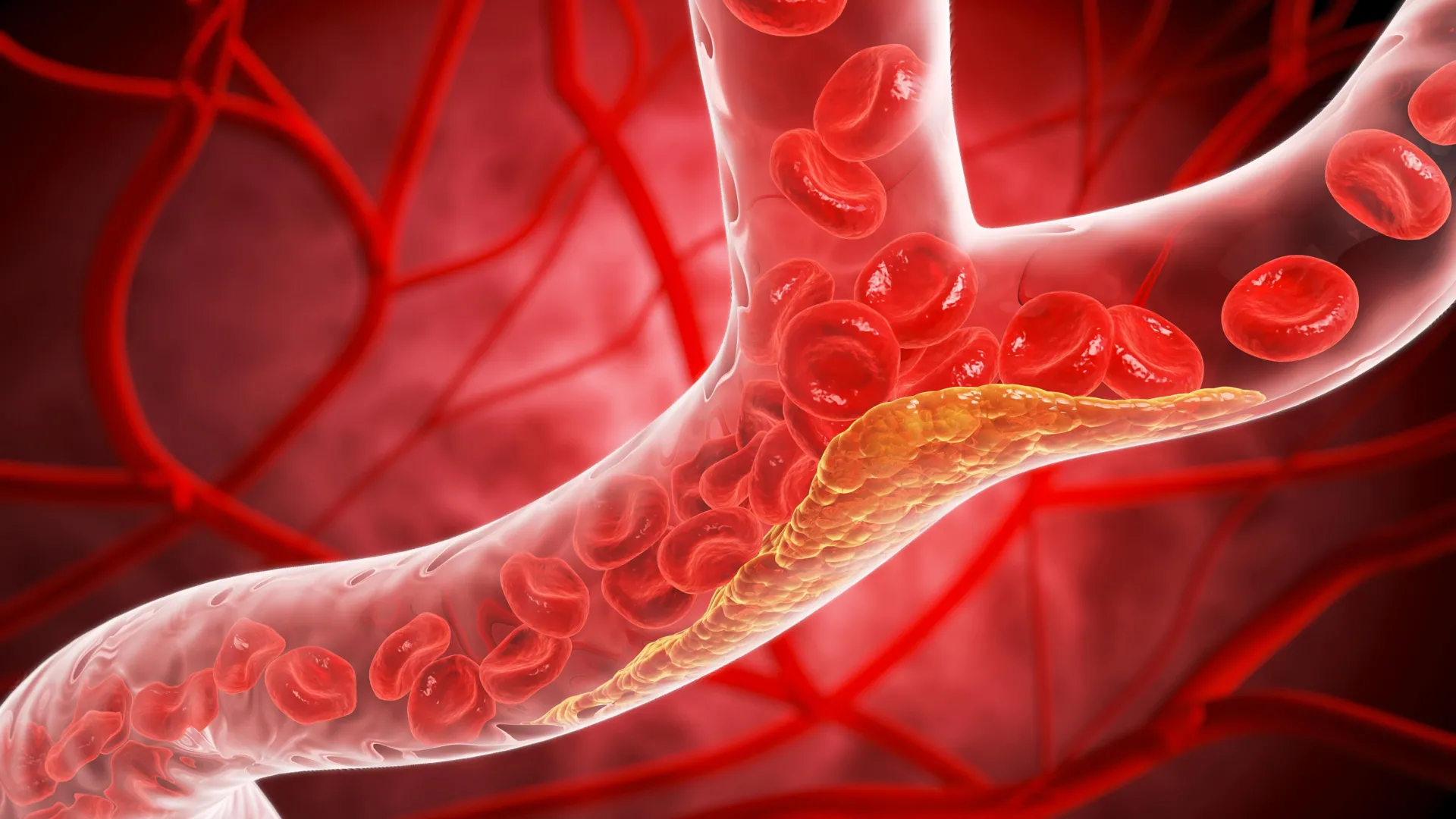
The 2026 guidelines underscore a clear, evidence-based mantra: when it comes to LDL (low-density lipoprotein) cholesterol, lower is better. The committee has reaffirmed that reducing LDL levels is the most effective strategy for preventing the buildup of plaque that leads to life-threatening vascular events.
Evolving Treatment Targets
The updated clinical thresholds provide a tiered approach to treatment:
- Optimal Health: For those without existing cardiovascular disease, the target remains below 100 mg/dL.
- Intermediate Risk: Clinicians are advised to drive levels below 70 mg/dL.
- High-Risk Individuals: A more aggressive target of less than 55 mg/dL is recommended, with some experts suggesting even lower thresholds for those with advanced atherosclerosis.
Addressing Lp(a) and Genetic Risk
A significant addition to this year’s guidance is the formal inclusion of lipoprotein(a), or Lp(a), as a measurable risk factor. Lp(a) is largely genetically determined, and elevated levels can significantly increase the risk of heart disease. The guidelines recommend a one-time screening for Lp(a) to identify individuals at higher baseline risk, allowing for earlier and more targeted preventive care. For those with familial hypercholesterolemia, the guidelines now recommend screening to begin as early as age 9, ensuring that genetic predispositions are managed before significant arterial damage can occur.
Official Responses and Expert Perspective
The leadership behind the guidelines emphasizes that these changes are designed to empower both patients and providers. Dr. Roger S. Blumenthal, chair of the guideline writing committee and director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, notes that the goal is to establish "optimal heart and vascular health throughout a person’s life."
"We know that bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life," Dr. Blumenthal stated during the presentation in New Orleans. His colleague, Dr. Seth Martin, echoed this sentiment, emphasizing that the "paradigm shift toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease and lead to better health outcomes for people decades later."
The Pillars of Prevention: Lifestyle Still Reigns Supreme
Despite the advanced pharmacological options and high-tech screening tools introduced in the 2026 update, the committee was careful to reiterate that medication is only part of the solution. Roughly 80% to 90% of cardiovascular disease remains linked to modifiable lifestyle factors.
The guidelines reaffirm the "foundational five" of heart health:
- Nutritional Integrity: Adhering to a balanced, heart-healthy diet.
- Physical Activity: Regular, consistent exercise to maintain vascular tone.
- Tobacco Cessation: Complete avoidance of nicotine products.
- Sleep Hygiene: Recognizing the critical role of rest in metabolic health.
- Weight Management: Maintaining a healthy body mass to reduce systemic inflammation.
These lifestyle modifications are the first line of defense. The guidelines position pharmacological interventions—such as statins, ezetimibe, bempedoic acid, and PCSK9 inhibitors—as essential tools to be used in conjunction with, not as a replacement for, these fundamental lifestyle changes.
Implications for Clinical Practice and Future Research
The 2026 guidelines have significant implications for how primary care physicians and cardiologists will manage patient health in the coming years. By broadening the scope of screening to include younger adults and complex risk factors, the guidelines demand a more comprehensive and personalized approach to the patient encounter.
Tailoring Care for Vulnerable Populations
The update provides specific guidance for groups that were previously underserved by general recommendations, including pregnant or breastfeeding individuals, the elderly (75+), and patients living with chronic conditions such as HIV, cancer, or advanced kidney disease. By providing tailored protocols for these groups, the ACC and AHA are ensuring that no patient is left behind in the effort to reduce cardiovascular morbidity.
A Look Toward the Future
The inclusion of imaging tools, such as coronary artery calcium (CAC) scans, provides clinicians with the ability to visualize the presence of plaque directly. These "risk enhancers" serve as a bridge between assessment and treatment, allowing for shared decision-making that is rooted in objective, physiological evidence.
As the field looks ahead, the influence of the VESALIUS-CV trial is expected to grow. The results of that trial suggest that even more aggressive lowering of LDL-C—potentially below 55 mg/dL—will become the gold standard for high-risk patients. The 2026 guidelines have set the stage for this evolution, creating a flexible, data-driven framework that can adapt as new therapies and clinical trials continue to emerge.
In conclusion, the 2026 ACC/AHA cholesterol guidelines represent a sophisticated, patient-centered approach to one of the most critical health challenges of our time. By prioritizing early detection, leveraging the power of big data through the PREVENT calculator, and embracing a personalized approach to pharmacological and lifestyle management, the medical community is now better equipped than ever to turn the tide against cardiovascular disease. The message is clear: the path to a healthier heart is no longer a distant goal for the elderly, but a continuous, proactive commitment that begins long before the first sign of trouble.