








In the landscape of modern cardiovascular medicine, clinicians are increasingly confronted with a silent epidemic: the catastrophic intersection of methamphetamine use and acute myocardial infarction (MI). While the medical community has long been vigilant regarding the risks of cocaine-induced cardiac events, a new, comprehensive study from California suggests that methamphetamine—a potent and highly addictive synthetic stimulant—is a significantly more prevalent driver of heart attacks in younger adults than previously realized.
According to research recently published in the Journal of the American Heart Association, approximately one in six heart attacks among adults under the age of 65 may be directly linked to methamphetamine use. This discovery challenges conventional diagnostic pathways and highlights a critical gap in public health awareness, where even “casual” users are unknowingly placing their cardiovascular health at extreme risk.
Main Facts: A Cardiovascular Crisis
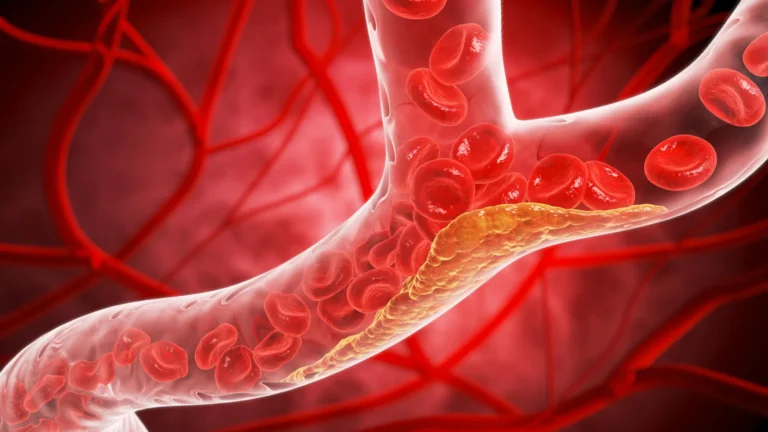
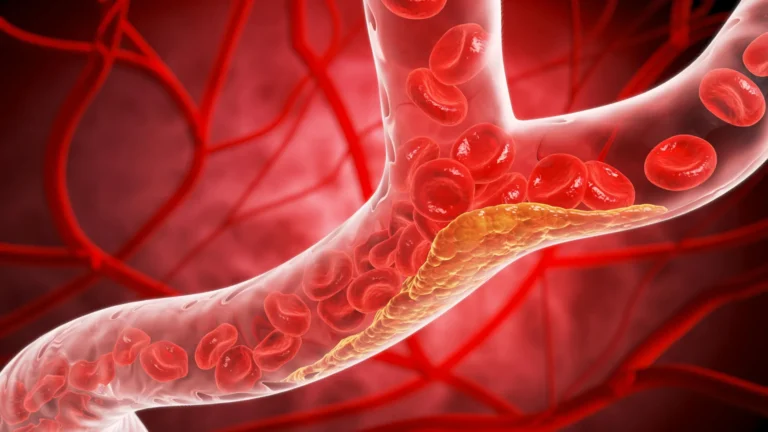
The study, led by Dr. Susan X. Zhao of the Santa Clara Valley Medical Center in San Jose, California, sheds light on the physiological mechanisms through which methamphetamines wreak havoc on the heart. Unlike traditional heart disease driven by long-term cholesterol buildup, meth-associated cardiac events are often driven by acute, systemic stressors.
The drug acts as a powerful vasoconstrictor, causing a rapid and dangerous spike in blood pressure. This, coupled with acute vasospasm—the sudden tightening of coronary arteries—and the accelerated development of premature coronary atherosclerosis, creates the perfect storm for a myocardial infarction.
The findings are stark: methamphetamine users are not only more likely to suffer an MI at a younger age but are also more likely to experience fatal outcomes compared to their non-using counterparts. Perhaps most alarmingly, the study indicates that many of these patients present with nonobstructive coronary artery disease (CAD), a condition that may not always align with traditional treatment protocols for heart attacks, further complicating clinical management.
Chronology: A Decade of Data Analysis
To arrive at these findings, researchers conducted a retrospective analysis of electronic medical records spanning a decade, from 2012 to 2022. The study focused on a cohort of 1,309 patients aged 18 to 65 who presented at Santa Clara Valley HealthCare with acute coronary syndrome (ACS) due to presumed type I myocardial infarction. All subjects underwent coronary angiography to provide a clear picture of their arterial health.
By filtering out cases involving cocaine use or non-type 1 MI, the researchers isolated 194 patients (14.8%) whose heart attacks were categorized as methamphetamine-associated. The identification of these cases was rigorous, relying on a combination of self-reported use and positive urine toxicology screenings conducted during the index hospitalization.
This ten-year window provides a longitudinal view of how the regional methamphetamine crisis has translated into hospital admissions, revascularization procedures, and, tragically, mortality.
Supporting Data: The Profile of Risk
The comparative data between methamphetamine-associated MI patients and the control group reveals a profile of distinct socioeconomic and clinical disparities.
Clinical Characteristics
- Age and Biology: Methamphetamine users in the study were younger, with a median age of 52 compared to 57 for the non-user group. Their left ventricular ejection fraction (LVEF)—a measurement of the heart’s pumping efficiency—was significantly lower (median 50% vs. 55%).
- The Anatomy of the Attack: One of the most notable findings was the prevalence of nonobstructive CAD. Meth users were more than twice as likely to have nonobstructive disease (24.3% vs. 10.6%), which resulted in a lower likelihood of undergoing revascularization procedures (59.3% vs. 75.0%).
- Comorbidities: While rates of hypertension and obesity remained similar across both groups, meth users were significantly more likely to smoke cigarettes (71.6% vs. 21.6%) and consume alcohol (28.9% vs. 8.3%). Conversely, they were less likely to have diabetes and tended to exhibit more favorable lipid profiles, suggesting that the cardiac events were driven more by the acute chemical toxicity of the drug than by traditional metabolic disease.
Social Determinants of Health
The study highlighted a profound social dimension to this medical crisis. Methamphetamine-associated MI patients were eight times more likely to be experiencing homelessness (25.8% vs. 3.2%) than their non-using counterparts. These findings suggest that the cardiovascular burden of methamphetamine use is inextricably linked to broader social determinants of health, complicating the ability of clinicians to provide effective long-term care and secondary prevention.

Official Responses and Clinical Perspectives
Dr. Susan X. Zhao noted that the findings were a surprise, even to the research team. However, she emphasized that the data likely reflects the high regional prevalence of methamphetamine use in Northern California rather than a singular nationwide pattern.
"Patients often express surprise when they learn their MI might be related to meth use," Dr. Zhao remarked. "Because much of that use is casual enough that it doesn’t register as an addiction, they don’t see the danger." She recalled instances where patients would admit to daily use while simultaneously expressing complete ignorance of the cardiovascular consequences.
The medical community, Dr. Zhao argues, must pivot its approach. "For this particular segment of MI patients, ‘stop using methamphetamines’ should be as important a part of your secondary prevention as everything else," she stated, noting that current discharge instructions often focus on traditional lifestyle changes—such as diet and exercise—that fail to address the root cause of the injury in these specific patients.
Implications for Public Health and Policy
The implications of this study extend far beyond the emergency room. The data suggests that methamphetamine-associated heart disease creates a "hidden" economic and societal burden that is not currently accounted for in national health statistics.
A Call for Targeted Prevention
The high rate of readmissions for subsequent ACS events (42.3% for users vs. 27.2% for nonusers) underscores the failure of the current system to engage these patients in meaningful addiction treatment. If a patient is treated for an MI but their substance use disorder remains unaddressed, the likelihood of a recurring, and potentially fatal, event remains high.
The Need for Multicenter Research
The authors acknowledge that their study captures only the "numerator"—those patients who were sick enough to require angiography. The "denominator"—the total population of individuals living with methamphetamine-induced cardiac damage who have yet to reach the stage of acute infarction—remains unknown. Addressing this will require large-scale, multicenter registry data to define the true scope of "meth-angina" spectrum disease.
Policy Reform
Ultimately, Dr. Zhao asserts that clinical interventions alone will not suffice. "Public policy will have to change," she stated, emphasizing that the intersection of addiction, homelessness, and heart disease requires a systemic approach. The research team is now shifting their focus to quantify the financial burden of methamphetamine-related heart failure, a move intended to provide policymakers with the hard data necessary to allocate resources more effectively.
Conclusion
The study from Santa Clara Valley Medical Center serves as a clarion call for the medical community to broaden its diagnostic lens. When a younger adult presents with an acute myocardial infarction, clinicians must consider the possibility of methamphetamine use, even in the absence of traditional risk factors.
As the usage of synthetic stimulants continues to rise across the United States, the healthcare system must evolve to meet the challenge. This means integrating addiction counseling into cardiovascular care, destigmatizing the conversation around substance use in clinical settings, and developing comprehensive public health strategies that address the social and physiological roots of this growing crisis. Failure to act will not only result in more frequent hospital readmissions but will continue to cost countless lives among a younger, vulnerable population.