






The landscape of cardiac rhythm management is on the cusp of a significant procedural evolution. For years, the subcutaneous implantable cardioverter defibrillator (S-ICD) has been heralded as a safer, less invasive alternative to traditional transvenous ICDs, particularly in reducing lead-related complications. However, a persistent "logistical hurdle"—the mandatory defibrillation testing (DFT) performed post-implantation—has remained a point of contention.
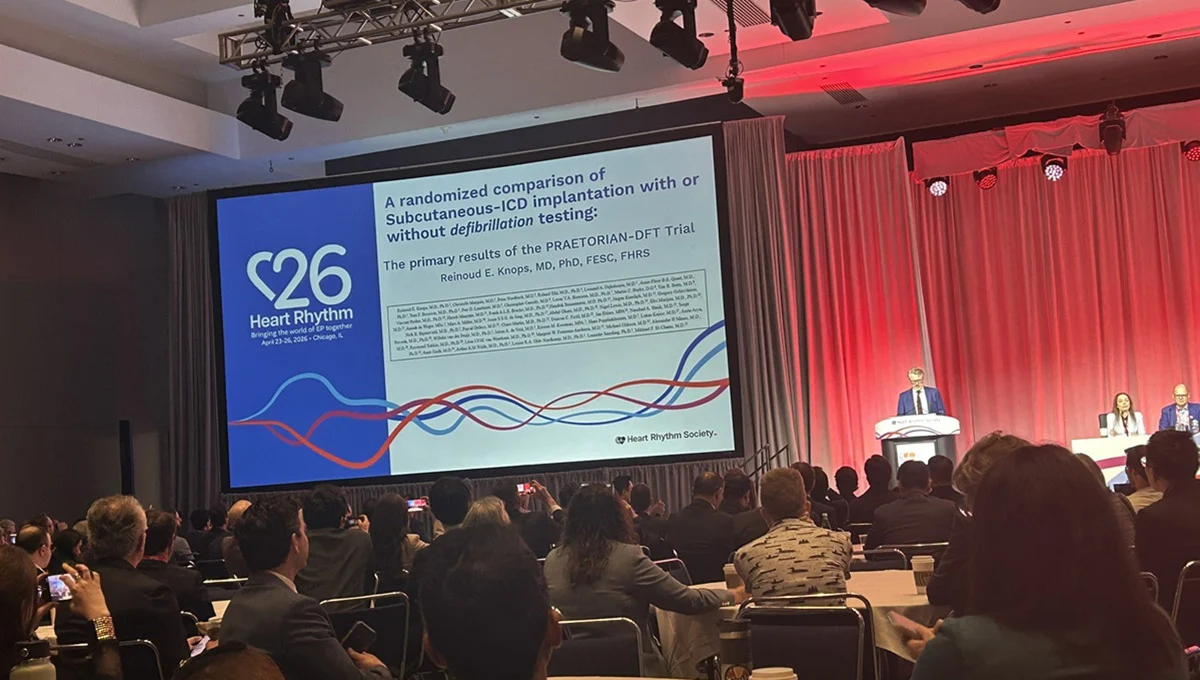
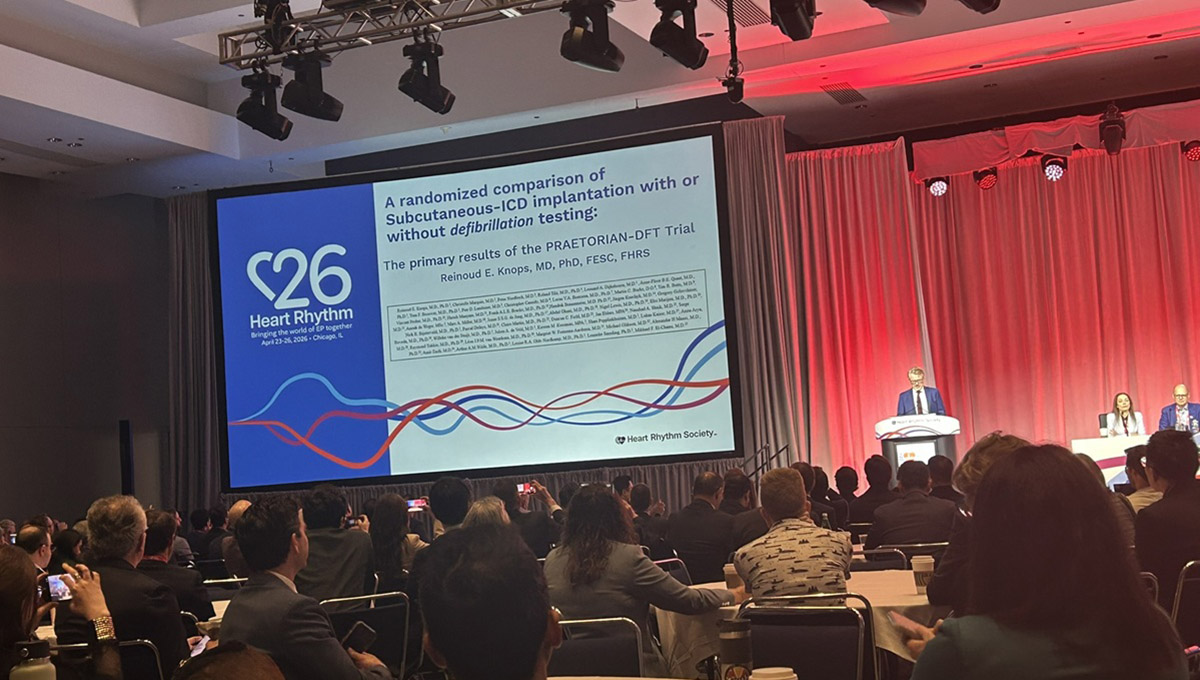
New findings from the randomized PRAETORIAN-DFT trial, presented at Heart Rhythm 2026, suggest that this step, which requires sedation or general anesthesia, may be largely unnecessary when a standardized radiographic scoring system is utilized. The results, published simultaneously in Circulation, indicate that omitting DFT not only maintains patient safety but also reduces procedural complications, potentially clearing the path for broader adoption of the S-ICD.
The Main Facts: Simplifying the S-ICD Workflow
The PRAETORIAN-DFT trial set out to determine whether physicians could safely forgo the traditional practice of inducing a ventricular arrhythmia under anesthesia to confirm that a newly implanted S-ICD could successfully terminate the rhythm.
The trial compared two strategies: a standard-of-care arm involving routine DFT and a "no-DFT" arm, where testing was omitted if the device’s position met specific criteria on a post-implant chest X-ray, as determined by the PRAETORIAN score. The results were compelling: the rate of failed first shocks for spontaneous ventricular arrhythmias—the trial’s primary endpoint—was 1.7% in the no-DFT group and 2.3% in the DFT group. This difference met the rigorous statistical criteria for noninferiority, confirming that the no-DFT approach is as effective as the traditional method.
Crucially, the trial found no difference in all-cause mortality between the two groups, and, perhaps most importantly, the no-DFT strategy was associated with fewer peri-procedural complications.
Chronology: From Transvenous Lessons to S-ICD Validation
To understand the weight of the PRAETORIAN-DFT findings, one must look at the historical trajectory of ICD implantation.
The Decline of DFT in Transvenous ICDs
For decades, DFT was considered the "gold standard" for confirming device efficacy. However, landmark trials such as SIMPLE and NORDIC ICD demonstrated that for transvenous ICDs, the risks associated with induction testing often outweighed the benefits. These trials effectively rendered routine DFT obsolete for transvenous devices, shifting the focus toward optimal lead placement through non-invasive means.
The Rise of the S-ICD
As S-ICDs gained traction, they were celebrated for avoiding the vascular space, thereby eliminating lead-related complications like endocarditis or vascular injury, as highlighted in the original PRAETORIAN and ATLAS S-ICD trials. Yet, because S-ICD efficacy is highly sensitive to the physical orientation and position of the device relative to the heart, professional societies—including the Heart Rhythm Society and the European Heart Rhythm Association—continued to issue strong recommendations for mandatory DFT.
The Development of the PRAETORIAN Score
Recognizing the burden of anesthesia and the inherent risks of testing, investigators led by Dr. Reinoud Knops at the Amsterdam University Medical Centre developed the PRAETORIAN score. By analyzing the device’s position on a simple chest X-ray, the score provides a reliable predictor of defibrillation success. Validation studies showed that a score below 90 predicted success with greater than 99% accuracy, setting the stage for the PRAETORIAN-DFT trial to test this hypothesis in a real-world, multicenter clinical setting.
Supporting Data: Examining the Trial Architecture
The PRAETORIAN-DFT trial was a robust, international endeavor, involving 965 patients across 37 centers in Europe, the United States, and Israel. The study population was diverse, with a mean age of 54 years and a significant representation of women (24%). The patient cohort was split between ischemic (45%) and nonischemic (35%) cardiomyopathies, with a mean left ventricular ejection fraction (LVEF) of 40%.
Primary and Secondary Outcomes
The primary endpoint—failed first shocks for spontaneous ventricular tachycardia or fibrillation—was achieved at low rates in both groups. The "no-DFT" arm actually trended toward superior performance in terms of shock efficacy, though the difference was statistically nonsignificant.
Safety metrics, however, painted a clearer picture. While the DFT group experienced a 1.7% incidence of DFT-related complications, the no-DFT group experienced none. Furthermore, composite complications within the first 30 days were significantly lower in the no-DFT cohort (1.7% vs. 4.8%). Dr. Knops pointed out that these complications, including unplanned ICU stays and cardiac decompensation, suggest that the procedure of DFT itself poses an unnecessary physiological stressor to patients who are often already fragile.
Official Responses and Expert Commentary
The medical community has received the trial results with cautious optimism, acknowledging that the data provide a much-needed evidence base for changing clinical behavior.
Dr. Reinoud Knops, the study’s lead investigator, emphasized the shift in perspective: "Defibrillation testing can be safely omitted after S-ICD implantation when guided by the PRAETORIAN score. This simplifies the procedure and potentially increases S-ICD adoption."
The "Medicolegal" Necessity for Updated Guidelines
Dr. Andrea Russo, a discussant at Heart Rhythm 2026 from the Cooper Medical School of Rowan University, provided critical context. She noted that many clinicians have already begun to abandon routine DFT in favor of fluoroscopy and impedance testing, often driven by patient comfort and procedural efficiency.
"This has potential medicolegal implications," Dr. Russo noted, highlighting the tension between existing, outdated professional guidelines and the reality of modern clinical practice. "These guidelines absolutely need to be updated. This is a well-conducted study that addresses a really important gap in our knowledge and should change our practice."
Implications: A New Era for Cardiac Implantable Devices
The implications of the PRAETORIAN-DFT trial are far-reaching, affecting everything from hospital logistics to patient quality of life.
Clinical Workflow and Accessibility
By removing the requirement for DFT, the S-ICD implant procedure becomes faster, requires less anesthesia, and can potentially be performed in a wider array of clinical settings. This lowers the barrier to entry for both physicians—who may be deterred by the technical and anesthetic demands of testing—and patients, who often fear the prospect of induced arrhythmias and the associated recovery.
The Future of Guideline Development
The call for updated guidelines is unlikely to go unheeded. With the weight of the PRAETORIAN-DFT evidence, professional societies are now under pressure to revise their consensus statements. This transition will likely shift the emphasis from "testing by induction" to "testing by image verification."
Unanswered Questions and Future Research
Despite the positive findings, experts like Dr. Russo have pointed to areas requiring further exploration. Questions remain regarding:
- High-Score Management: How should clinicians manage the small subset of patients who do not meet the low-score threshold?
- Technique Standardization: Will the industry adopt the PRAETORIAN score as a universal standard, or will individual centers continue to rely on proprietary imaging techniques?
- Generalizability: Will the results hold true across the full spectrum of S-ICD implanters, including those in less specialized community settings?
Conclusion
The PRAETORIAN-DFT trial represents a landmark moment in electrophysiology. By demonstrating that high-quality radiographic assessment can replace the archaic and risky practice of routine defibrillation testing, the study offers a clear path toward a more efficient, safer, and more accessible future for S-ICD patients. As the medical community moves to digest these findings, the focus must now shift toward the rapid integration of the PRAETORIAN score into standard clinical protocols, ensuring that the technology designed to protect patients from sudden cardiac death is as easy to implement as it is effective to use.