









For the first time since 2018, the American College of Cardiology (ACC) and the American Heart Association (AHA) have issued a comprehensive overhaul of clinical guidance for the screening and management of blood cholesterol. Unveiled on March 28 at the ACC’s 75th Annual Scientific Session in New Orleans and published concurrently in the Journal of the American College of Cardiology and Circulation, these guidelines represent a fundamental shift in how medicine addresses the silent, progressive threat of cardiovascular disease (CVD).
The release, which arrives in tandem with a foundational paper in the American Journal of Preventive Cardiology titled "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026," signals a move away from "one-size-fits-all" management toward a strategy of aggressive, personalized, and early-intervention cardiology.
The Evolution of Prevention: A Chronological Context
The landscape of cardiovascular care has shifted dramatically over the past decade. In 2018, the previous guidelines established a robust framework for statin therapy and risk stratification. However, the last eight years have seen an explosion in genetic research, the advent of potent new injectable therapies, and a growing realization that cardiovascular health is a lifelong continuum rather than a condition that suddenly appears in middle age.
The 2026 guidelines are the culmination of years of data synthesis, reflecting a proactive shift in the clinical paradigm. By integrating modern big-data analytics—most notably through the new PREVENT risk calculator—the 2026 update acknowledges that the "ticking clock" of atherosclerosis begins long before the first clinical symptom presents itself.
Core Pillars of the 2026 Recommendations
The updated guidance centers on a more granular approach to lipid management, focusing specifically on low-density lipoprotein (LDL) cholesterol and the often-overlooked Lipoprotein(a), or Lp(a).
The Shift Toward Precision Cardiology
The new guidelines emphasize that clinicians must look beyond standard age-based thresholds. Personalized risk assessment is now the gold standard, requiring physicians to factor in a patient’s unique history. This includes:
- Family History: A deeper dive into hereditary patterns of atherosclerosis.
- Inflammatory Markers: Using high-sensitivity C-reactive protein (hsCRP) to gauge silent vascular inflammation.
- Life-Course Events: Recognizing that events like early menopause, preeclampsia, or gestational diabetes are independent risk factors for future heart disease.
Aggressive LDL Targets
The guidance establishes clear, tiered targets for LDL-C reduction, reflecting the mantra that "lower is better" when it comes to cardiovascular longevity:
- General Population: Aiming for levels below 100 mg/dL.
- Intermediate Risk: Targeted levels below 70 mg/dL.
- High-Risk Individuals: A more aggressive target of less than 55 mg/dL.
Supporting Data: Why the Shift is Necessary
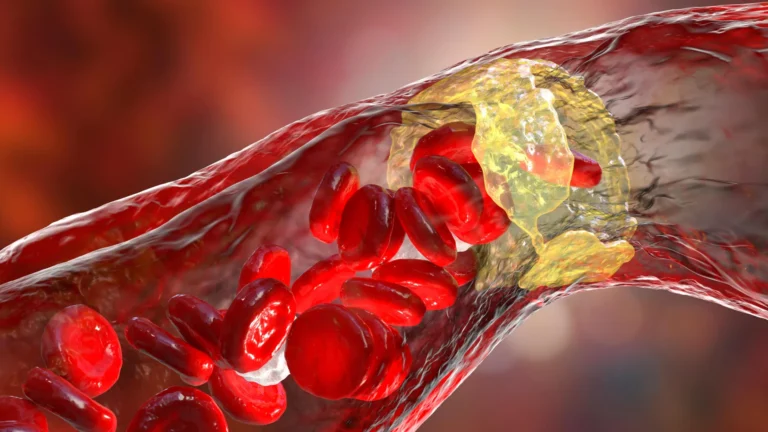
The urgency of these guidelines is underscored by sobering statistics: approximately 1 in 4 U.S. adults currently lives with elevated LDL cholesterol. This condition is the primary driver of atherosclerosis, the slow buildup of plaque within the artery walls that restricts blood flow. When this plaque becomes unstable, it can rupture, leading to myocardial infarction (heart attack) or stroke.
The Power of the PREVENT Calculator
Perhaps the most significant technical advancement in the 2026 update is the introduction of the Predicting Risk of Cardiovascular Disease EVENTs (PREVENT) calculator. Unlike its predecessor, which relied on a smaller dataset of 26,000 individuals and focused on 10-year risk for those over 40, the PREVENT tool is built upon data from 6.6 million people.
By incorporating kidney function and blood sugar levels, and by allowing for risk estimation starting as early as age 30, the PREVENT tool provides a 30-year outlook. This longitudinal perspective allows clinicians to identify "at-risk" patients decades before a crisis occurs, enabling earlier lifestyle and pharmacological interventions.
Genetic Risks: The Case of Lp(a) and Familial Hypercholesterolemia
The guidelines now advocate for a one-time screening for Lipoprotein(a). Elevated Lp(a) levels—an inherited trait—are associated with a 40% increase in heart disease risk at 125 nmol/L, with that risk doubling at 250 nmol/L. Furthermore, those with familial hypercholesterolemia, a genetic condition causing severe LDL elevation, are now encouraged to begin screening as early as age 9.
Official Responses and Expert Commentary
Dr. Roger S. Blumenthal, chair of the guideline writing committee and director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, emphasized the physiological necessity of early action. "We know that lower LDL cholesterol levels are better when it comes to reducing the risk of heart attacks, strokes, and congestive heart failure," Dr. Blumenthal stated. "Bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life."
Dr. Seth Martin, a cardiologist and committee member, highlighted the philosophical shift toward "proactive prevention." According to Dr. Martin, "Shifting the paradigm toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease and lead to better health outcomes for people decades later."
The Enduring Role of Lifestyle
Despite the technological and pharmacological advancements, the guidelines reiterate that 80% to 90% of cardiovascular disease remains linked to modifiable factors. The foundation of heart health remains:
- A nutrient-dense, balanced diet.
- Consistent, moderate-to-vigorous physical activity.
- Complete cessation of tobacco use.
- Prioritizing sleep hygiene and weight management.
The guidelines frame these lifestyle changes not as an alternative to medicine, but as the essential first step upon which all other therapeutic interventions are built.
Implications for Patient Care and Future Research
The 2026 guidelines significantly expand the toolkit available to clinicians. Beyond traditional statins, the document provides clear clinical pathways for:
- Ezetimibe and Bempedoic Acid: Providing options for patients who are statin-intolerant or require supplemental lipid-lowering.
- PCSK9 Monoclonal Antibodies: An essential addition for high-risk patients requiring rapid, substantial reductions in LDL-C.
- Special Populations: Dedicated sections provide guidance for pregnant/breastfeeding individuals, cancer survivors, patients with HIV, and those with advanced kidney disease.
Looking Toward the Future: The VESALIUS-CV Influence
The release of these guidelines is not an end point but a baseline. In an accompanying editorial, experts pointed to the findings of the VESALIUS-CV clinical trial, which demonstrated the long-term benefits of aggressive, multi-therapy cholesterol reduction. There is a strong consensus that future iterations of these guidelines may push the target for moderate atherosclerosis patients even further, potentially setting the standard at below 55 mg/dL across a broader swathe of the population.
Conclusion
The 2026 clinical guidance represents a maturation of cardiovascular medicine. By moving from a reactive model that treats disease after it manifests to a proactive model that identifies and mitigates risk in the prime of life, the ACC and AHA have provided a blueprint for a healthier future. For the patient, this means more personalized, data-driven conversations with their care team. For the clinician, it offers a sophisticated, evidence-based roadmap to prevent the "silent epidemic" of heart disease before it can claim another life.
As medicine continues to evolve, the integration of genetic screening, big-data risk modeling, and advanced pharmacotherapy ensures that the fight against cardiovascular disease is increasingly weighted in favor of the patient. Through this collaborative effort, the American College of Cardiology and the American Heart Association have set a new standard of care that prioritizes long-term wellness over short-term symptom management.