






In the landscape of modern medicine, few conditions are as pervasive, destructive, and misunderstood as substance use disorder (SUD). Addiction medicine—a field dedicated to the prevention, evaluation, diagnosis, and treatment of those suffering from addiction—has long been siloed as a niche practice. While the American Board of Medical Specialties (ABMS) officially recognized addiction medicine as a formal subspecialty in October 2015, the escalating crisis of the overdose epidemic suggests that confining care to a handful of "specialists" is a strategy that is failing to meet the magnitude of the challenge.
With more than 40 million Americans—approximately 14.5 percent of the adult population—grappling with substance use issues, addiction is no longer a peripheral concern. It is a fundamental public health crisis that infiltrates every medical office, emergency room, and primary care clinic in the country. To address this, the medical community must pivot toward a universal standard of care: integrating addiction screening and intervention into every patient encounter, regardless of the provider’s specialty.
The Evolution of a Subspecialty: A Brief Chronology
The formalization of addiction medicine has been a slow climb toward recognition. For decades, the medical establishment treated addiction as a moral failing or a behavioral issue rather than a chronic disease requiring physiological intervention.
- Pre-2015: Addiction treatment was largely handled by specialized rehabilitation centers and a small cadre of dedicated psychiatrists. Most physicians received little to no formal training on the pathology of addiction, leading to a gap in care that left millions of patients without support during routine medical visits.
- October 2015: The ABMS officially recognized addiction medicine as a subspecialty. This marked a watershed moment, providing a framework for board certification and standardized training. However, it inadvertently created a psychological barrier, signaling to the broader medical community that "if you aren’t a specialist, this isn’t your patient."
- April 2021: In response to the surging opioid crisis, the Department of Health and Human Services (HHS) moved to lower barriers for prescribing buprenorphine, a life-saving partial opioid agonist. This signaled a shift in federal policy, moving toward the "democratization" of addiction treatment by allowing more non-specialist clinicians to participate in essential care.
- Present Day: Despite these policy shifts, the integration of addiction medicine into standard clinical curricula remains sluggish, with most residency programs still failing to prioritize the subject.
The Data: A Crisis of Unprecedented Scale
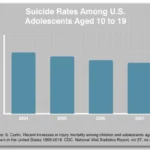
The numbers tell a story of a system currently overwhelmed. According to the CDC’s National Center for Health Statistics, the 12-month period ending in April 2021 saw an estimated 100,306 drug overdose deaths in the United States—a harrowing 28.5 percent increase from the previous year. Within that statistic, opioid-related deaths accounted for nearly 76,000 lives, a 35 percent spike.
The disparity between the prevalence of the disease and the availability of trained clinicians is stark. Research published in the journal Substance Abuse revealed that only 24 percent of residency programs across the nation dedicate 12 or more hours of their total curriculum to addiction medicine. Consequently, the Association of American Medical Colleges (AAMC) reports that only about 3,100 medical professionals in the U.S. possess the specialized training necessary to treat the millions of Americans suffering from SUD.
Before the 2021 HHS policy changes, only about 6 percent of active physicians held the DEA’s "X-waiver," which was the legal prerequisite for prescribing buprenorphine. This administrative bottleneck created a "treatment desert" for patients who could have otherwise been stabilized in a primary care setting.
SBIRT: A Universal Clinical Tool
The most effective weapon against the addiction epidemic is not a new surgical procedure or a blockbuster drug, but a standardized clinical protocol known as SBIRT: Screening, Brief Intervention, and Referral to Treatment.
SBIRT is an integrated, evidence-based approach designed to identify individuals with substance use issues—or those at risk of developing them—at the earliest possible stage. The philosophy behind SBIRT is simple yet revolutionary: Why would we treat a patient for hypertension or diabetes without asking about their lifestyle and substance use?
The Clinical Imperative of Screening
Medical professionals routinely check for drug allergies, family history of heart disease, and immunization status. Ignoring substance use is a critical blind spot. By incorporating brief, non-judgmental screening questions into standard intake forms, physicians can:
- Identify risks early: Catching problematic use before it evolves into a chronic, life-threatening disorder.
- Mitigate Stigma: When a doctor asks about substance use as casually as they ask about blood pressure, it signals that the office is a "safe space." This reduces the shame that often prevents patients from seeking help.
- Facilitate Referral: Providing a clear, documented path to treatment allows the patient to feel supported rather than judged, significantly increasing the likelihood of successful recovery.
Official Responses and the Need for Curricular Reform
The medical establishment has been slow to mandate addiction education. For many physicians practicing today, their training consisted of a single lecture—or none at all—on the biology of addiction. This "education gap" is a policy failure that must be corrected at the level of medical school and residency accreditation.

If the goal is to stem the tide of overdose deaths, the "specialist-only" model is insufficient. Medical schools must move toward a curriculum that treats addiction with the same academic rigor as oncology or cardiology. This means requiring clinical rotations in addiction settings and ensuring that every graduate is proficient in prescribing medications for opioid use disorder (MOUD).
The 2021 HHS decision to expand buprenorphine access was a necessary step, but it is only the beginning. True systemic change requires that addiction education be moved from an elective "interest area" to a core competency required for medical licensure.
Implications: A Shift in the Medical Paradigm
The implications of failing to integrate addiction medicine are clear: we will continue to see mortality rates climb as the medical system remains reactive rather than proactive. Conversely, if we empower the generalist workforce to manage SUDs, the implications for public health are profound.
1. The Humanization of Care
When doctors are trained to view addiction as a chronic, treatable disease, the patient-provider relationship shifts. The patient is no longer a "frequent flyer" or a "difficult case," but a human being managing a complex condition. This empathy is the cornerstone of effective treatment.
2. Economic and Social Benefits
The cost of untreated addiction is astronomical, affecting everything from workplace productivity to the overburdening of emergency services and the criminal justice system. Integrating treatment into routine medical care reduces the strain on these systems, shifting the focus from crisis management to disease prevention and maintenance.
3. Resilience and Recovery
Despite the grim statistics, there is hope. Addiction is one of the few medical conditions where "recovery" is a realistic and attainable goal for many. By providing patients with the tools, medication, and clinical support they need, physicians can facilitate long-term remission. This resilience is a testament to the power of medical intervention.
Conclusion: A Call to Universal Action
The addiction crisis is often framed as a battle of individual will or a failure of social policy, but it is, at its core, a medical challenge. We cannot expect a handful of specialists to treat 40 million people. The solution lies in the hands of the entire medical community—from pediatricians and primary care physicians to surgeons and hospitalists.
Reflecting on his own training 35 years ago, one practitioner noted he received only a single hour of lecture on the subject. Today, he views his daily work with patients seeking recovery as a privilege. This shift in perspective—from viewing addiction as a "problem to avoid" to a "condition to treat"—is the essential evolution required for modern medicine.
We are all capable of assessing, intervening, and providing care. By dismantling the barriers of stigma and updating our educational standards, we can transform the landscape of addiction medicine, one patient at a time. The certificates on our walls may define our specialties, but our responsibility as healers extends to every patient who walks through our doors, particularly those who are the most vulnerable. It is time to treat addiction as the universal medical priority it truly is.