For years, the phrase "my ostomy bag saved my life" felt like a sentence the author, Tayler Goectau, couldn’t rightfully claim. In the landscape of chronic illness, ostomies are often categorized by "clear-cut" pathology: inflammatory bowel disease (IBD), colorectal cancer, or acute diverticulitis. These conditions provide clinicians with measurable metrics and a standard roadmap for intervention. However, for those living with Ehlers-Danlos syndrome (EDS)—a complex group of connective tissue disorders—the journey to the operating room is rarely linear, often marked by decades of gaslighting, diagnostic dead-ends, and debilitating, "invisible" gastrointestinal dysfunction.
This is the story of two years of living with an ostomy, the fight for medical legitimacy, and the realization that for many with EDS, the path to healing requires radical advocacy.
The Invisible Scaffolding: Understanding EDS and the Gut
Ehlers-Danlos syndrome is fundamentally a disorder of the body’s "scaffolding." Connective tissue, which provides structure and integrity to the skin, blood vessels, joints, and internal organs, is compromised in patients with EDS. While public awareness often centers on joint hypermobility or chronic pain, the multisystemic nature of the condition frequently impacts the gastrointestinal tract with devastating efficiency.
For those with EDS, the gut is not merely a digestive organ; it is a complex muscular system that relies on structural integrity to function. When that integrity is flawed, the result can be chronic dysmotility, severe constipation, and structural shifts that baffle standard GI specialists.
A Chronology of "Just Constipation"
The narrative of chronic illness is often told through a series of dismissed symptoms. For Goectau, the struggle was not a sudden onset of disease but a lifelong progression:

- Childhood and Adolescence: The symptoms began early—waves of abdominal pain in school hallways and the quiet, persistent struggle of chronic constipation that transformed into a source of adolescent shame.
- The Collegiate Toll: By college, the dysfunction had escalated into a lifestyle-altering disability. The fear of being away from a restroom forced an involuntary housebound existence.
- The Diagnostic Cascade: Traditional treatments—laxatives, dietary modifications, and standard motility tests—failed to provide relief. It was only when a specialist finally validated the severity of the situation that a "cascade of testing" began. This involved high-level imaging to identify structural anomalies that had been previously overlooked by clinicians who viewed the patient through the narrow lens of irritable bowel syndrome (IBS).
- The Surgical Turning Point: Following a decade of searching for answers, the decision to proceed with an end ileostomy was made. This procedure, which diverts waste from the small intestine into an external pouch, was deemed the only viable path to restore quality of life.
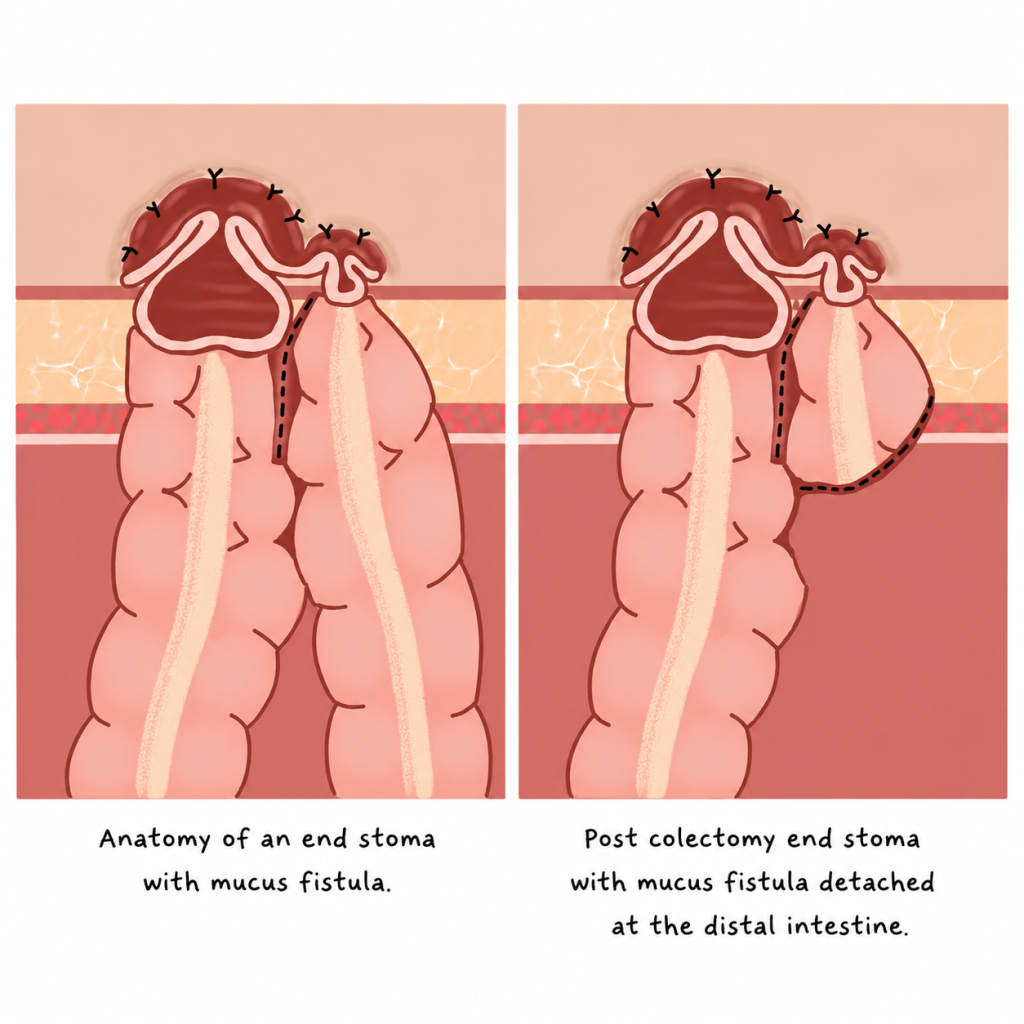
The Mechanics of the Procedure
To understand the gravity of the decision, one must understand the surgical reality. An ostomy creates a stoma—an opening in the abdominal wall. In Goectau’s case, the procedure was an end ileostomy. Unlike a loop ostomy, which is often temporary, this involved the removal of the colon—a total colectomy—to resolve the source of the patient’s severe, persistent dysmotility.
This was not a decision made lightly. It involved profound existential anxiety: Will I smell? Will it leak? How will this impact my identity? The fear of "contamination OCD" and the social stigma surrounding ostomy bags are significant barriers that keep many patients from seeking the very treatment that could return them to a functioning life.
The Reality of Recovery: An Unvarnished Perspective
The recovery from a total colectomy is rarely a linear trajectory, especially for an EDS patient whose tissues do not heal with the same predictability as the general population. The surgery itself, lasting over ten hours, was merely the first step.
"The recovery was not clean or linear," Goectau reflects. The process required constant self-advocacy from a hospital bed, managing post-operative complications, and navigating the psychological grief of losing a part of one’s anatomy. Yet, the outcome was transformative. The chronic bloating, the constant, crushing heaviness, and the fear of the next "episode" dissipated. The stoma became a functional tool for survival.
Implications for Medical Providers and Patients
The case of Tayler Goectau serves as a critical case study for the medical community. It highlights a recurring failure in modern medicine: the tendency to categorize symptoms as "functional" or "psychosomatic" simply because they do not appear on standard, low-resolution imaging.
For the Medical Provider:
- Listen to the Narrative: When an EDS patient presents with a lifetime of treatment-resistant GI dysfunction, consider the systemic nature of the connective tissue disorder.
- Think Structurally: Investigate potential visceroptosis (the downward displacement of organs) and advanced motility issues that standard "IBS" protocols cannot capture.
- Validate, Don’t Dismiss: The exhaustion of fighting for diagnostic clarity is a trauma in itself. Clinical bias against "invisible" patients directly hinders health outcomes.
For the Patient:
- Your Symptoms are Real: "Just constipation" is a minimizing term for a condition that can render a life unlivable.
- Advocacy is Essential: In rare or complex presentations, the patient is often the primary investigator. Do not fear bringing research to your surgeon or requesting a second opinion.
- Community is a Catalyst: The isolation of having an "unheard of" condition is the greatest hurdle. Connecting with support groups—even those that start small—can lead to shared resources and the confidence to push for better care.
Beyond the Bag: Turning Trauma into Advocacy
Two years post-surgery, the author’s life has expanded in ways that were once unimaginable. Beyond the personal recovery, Goectau has channeled the experience into a small business—hand-sewing aesthetic ostomy covers—and global advocacy. This year, work with Campaign 52 took the author to Kenya, providing ostomy education and supplies to women in specialized hospitals.
The transition from a patient trapped by their own body to an advocate traveling internationally highlights the central thesis of the journey: an ostomy is not an end; it is a redirection.
Conclusion: A New Standard of Living
The "Stoma-Versary" is more than a date on a calendar; it is a celebration of reclaimed agency. For those currently standing at the precipice of a life-altering surgery, the fear is natural. However, the path forward is not defined by the bag, but by the life that becomes possible once the debilitating weight of chronic illness is removed.
As the medical field continues to grapple with the complexities of EDS, the voices of patients like Tayler Goectau provide the necessary bridge between clinical data and the lived human experience. The message is clear: when standard care fails, radical solutions—and radical advocacy—are not just options; they are life-saving necessities.
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, visceroptosis, or ostomies. Discussion of diagnostic testing, surgical interventions, and treatment outcomes is provided for educational purposes only and should not be interpreted as medical advice. Readers should consult their healthcare team regarding their individual circumstances.