







For the first time since 2018, the medical landscape regarding cardiovascular prevention has shifted significantly. On March 28, 2026, the American College of Cardiology (ACC) and the American Heart Association (AHA) unveiled updated clinical guidance on the screening and management of blood cholesterol. Presented at the ACC’s 75th Annual Scientific Session in New Orleans and simultaneously published in the Journal of the American College of Cardiology and Circulation, these recommendations represent the most comprehensive update in nearly a decade.
The guidelines aim to move beyond "one-size-fits-all" medicine, urging clinicians to adopt a lifelong, personalized approach to cardiovascular health. By integrating advanced risk-prediction models, aggressive lipid-lowering targets, and early-intervention strategies, the medical community is signaling a departure from reactive care toward a proactive, life-course trajectory of heart disease prevention.
The Core Mandate: Lowering LDL and Embracing Personalized Risk
The fundamental message of the 2026 guidance is clear: when it comes to cholesterol, lower is better. The committee, chaired by Dr. Roger S. Blumenthal, director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, emphasized that sustained control of low-density lipoprotein (LDL) cholesterol—often termed "bad cholesterol"—is the bedrock of preventing heart attacks, strokes, and congestive heart failure.
The updated guidelines emphasize three primary shifts:
- Earlier Screening: Detecting dyslipidemia in younger adults, particularly those with a family history or genetic predispositions.
- Individualized Assessment: Moving beyond basic age-based models to incorporate comorbid conditions and unique life events.
- Aggressive Targets: Establishing lower lipid thresholds for patients based on their specific risk profile, rather than generalized population-based goals.
"We know that bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life," says Dr. Blumenthal. "It is about protecting the vessel wall from damage before it manifests as clinical disease."
A Chronology of Change: Why Now?
The release of these guidelines follows an intensive multi-year review of clinical data, culminating in the 2026 update. To understand the gravity of these changes, one must look at the recent evolution of cardiovascular science:
- 2018–2022: The medical community recognized the limitations of the previous 2018 cholesterol guidelines, which were increasingly viewed as insufficiently aggressive for high-risk patients. During this period, the emergence of potent therapies like PCSK9 inhibitors and bempedoic acid expanded the clinical toolbox.
- 2023–2025: Research into the "life-course" impact of lipids gained momentum. Studies confirmed that cumulative exposure to high LDL levels over decades is a primary driver of atherosclerosis.
- March 2026: The ACC/AHA unveil the new guidelines, coinciding with the publication of "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026" in the American Journal of Preventive Cardiology, which serves as a clinical companion to the main guidelines.
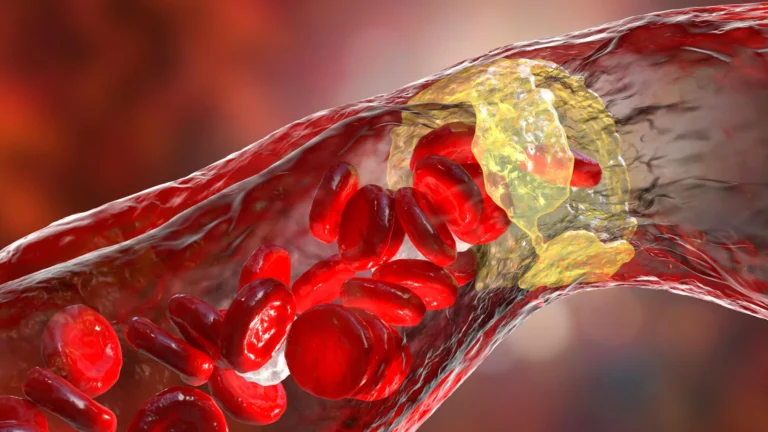
The urgency for these updates is underscored by a sobering statistic: approximately 25% of U.S. adults live with elevated LDL-C. This prevalence contributes to atherosclerosis, a silent killer where plaque builds up in artery walls, eventually restricting blood flow or triggering catastrophic ruptures.
Supporting Data: The Science Behind the Shift
The 2026 guidance is not merely an opinion piece; it is backed by an unprecedented volume of data. The most significant technical advancement is the PREVENT (Predicting Risk of Cardiovascular Disease EVENTs) calculator.
The Evolution of Risk Prediction
The previous risk assessment tools relied heavily on 10-year risk estimates for individuals 40 and older, using a limited set of variables: age, cholesterol, and blood pressure. The new PREVENT model, by contrast, is built on data from 6.6 million individuals—a massive increase over the 26,000 subjects used in previous iterations.
Key features of the PREVENT calculator include:
- Expanded Scope: The tool is designed to be used as early as age 30.
- Comprehensive Variables: It incorporates metabolic health markers, specifically kidney function and blood sugar levels, providing a more granular view of a patient’s systemic health.
- Long-Term Accuracy: It provides both 10-year and 30-year projections, allowing physicians to demonstrate to younger patients how their current lifestyle and lipid levels will likely impact their health decades into the future.
The Role of Genetic and "Hidden" Factors
The guidelines now place a greater emphasis on non-traditional markers. For instance, the recommendation for a one-time test for lipoprotein(a) [Lp(a)] is a major development. Lp(a) is an inherited factor that is largely unaffected by diet or exercise. High levels (125 nmol/L) increase heart disease risk by 40%, while levels of 250 nmol/L can double that risk. By identifying these markers early, clinicians can initiate intensive management strategies that were previously overlooked.
Official Responses and Clinical Implications
The medical community has reacted with cautious optimism, noting that while the guidelines increase the clinical workload, they provide the necessary framework to reduce the burden of cardiovascular disease.
Empowering the Patient-Clinician Dialogue
Dr. Seth Martin, a member of the guideline writing committee, stresses that the shift is as much about communication as it is about chemistry. "Shifting the paradigm toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease," he says. The guidelines encourage "shared decision-making," where the physician uses the PREVENT calculator not just as a diagnostic tool, but as a visual aid to help patients understand the "why" behind treatment recommendations.
Broadening the Treatment Toolbox
The guidelines provide specific, tailored advice for historically under-represented or complex populations, including:
- Pregnancy and Postpartum: Managing lipids in the context of gestational diabetes or preeclampsia.
- Chronic Illnesses: Specific protocols for patients with HIV, cancer, or advanced kidney disease.
- The Elderly: Refined guidance for those 75 and older, balancing the benefits of cholesterol-lowering therapies against the risks of polypharmacy.
Beyond traditional statins, the guideline validates the use of ezetimibe, bempedoic acid, and PCSK9 inhibitors. For patients who cannot tolerate high-dose statins or who require multi-drug therapy to reach their goals, these options have been elevated from "last-resort" status to standard-of-care recommendations.
The New Gold Standards: Lipid Targets
One of the most consequential aspects of the 2026 update is the explicit definition of "optimal" and "high-risk" targets:
- General/Low Risk: Maintain LDL-C below 100 mg/dL.
- Intermediate Risk: Lower LDL-C below 70 mg/dL.
- High Risk: Aim for levels below 55 mg/dL.
These targets are supported by findings from trials such as the VESALIUS-CV, which demonstrated that aggressive, sustained lipid reduction yields significant clinical benefits. The editorial accompanying the guidelines suggests that we are moving toward a future where 55 mg/dL might become the baseline for anyone with moderate evidence of plaque buildup (atherosclerosis).
A Call to Action: The Persistence of Lifestyle
Despite the advancements in pharmaceuticals and predictive analytics, the 2026 guidelines maintain a foundational truth: 80% to 90% of cardiovascular disease is linked to modifiable factors.
The guidelines do not abandon the basics. Instead, they reinforce them as the first line of defense:
- Nutritional Health: A balanced, heart-healthy diet.
- Physical Activity: Regular, sustained exercise.
- Habit Modification: Absolute cessation of tobacco use.
- Holistic Wellness: Prioritizing sleep hygiene and weight management.
"Lifestyle changes remain a critical first step," Dr. Blumenthal reiterated during the presentation in New Orleans. "Technology and medication are powerful, but they cannot replace the fundamental impact of daily habits on vascular health."
Conclusion: The Path Forward
The 2026 ACC/AHA guidelines represent a sophisticated evolution in preventive cardiology. By lowering the age of initial screening, integrating advanced genetic and metabolic markers, and setting more aggressive lipid targets, the medical community is attempting to "get ahead" of heart disease before it causes irreversible damage.
While the adoption of these guidelines will require a significant shift in clinical workflow—particularly regarding the widespread use of the PREVENT calculator and the inclusion of Lp(a) testing—the potential rewards are immense. By treating the patient as a whole, rather than a single lipid panel, clinicians can now offer a personalized roadmap for heart health that spans from young adulthood well into the later stages of life. As the medical community digests these new standards, the focus will now shift to implementation, ensuring that these life-saving strategies reach the patients who need them most.