




On Thursday, the Supreme Court of the United States issued a pivotal ruling preserving, at least temporarily, the accessibility of mifepristone—a key component in the standard two-drug medication abortion regimen—via telehealth and mail. While the decision provides a reprieve for reproductive health providers and patients across the country, it serves as only a temporary stabilization in a volatile legal landscape. As the case continues to wind its way through the lower courts, the medical community remains on high alert, bracing for a potential future where the gold standard of abortion care could be stripped away by judicial mandate rather than medical consensus.
The Legal Tug-of-War: A Chronology of Conflict
The current legal battle traces back to a high-stakes challenge spearheaded by the state of Louisiana. The state, which has already implemented a stringent abortion ban, argues that the availability of mifepristone via telehealth undermines its state-level regulations.
The conflict reached a fever pitch in April, when the 5th Circuit Court of Appeals issued a sudden and chaotic ruling that prohibited providers from remotely prescribing or mailing the medication. The 5th Circuit’s decision sought to reinstate the pre-2021 Risk Evaluation and Mitigation Strategies (REMS), which had historically barred the remote prescription of mifepristone.
The Food and Drug Administration (FDA) had lifted these restrictions in 2021, recognizing both the efficacy of the drug and the changing landscape of healthcare delivery during the Covid-19 pandemic. By siding with the lower court’s temporary reinstatement of these barriers, the 5th Circuit effectively signaled an intent to disrupt a widely adopted standard of care. Thursday’s Supreme Court decision reversed that order, staying the implementation of the 5th Circuit’s restrictions while the broader legal merits of the case are debated. However, the litigation is far from over, and the threat to telehealth access remains a looming specter over the American healthcare system.
Data and Efficacy: The Case for Telehealth
Since the overturning of Roe v. Wade in 2022, the demand for telehealth-based abortion services has surged, filling a critical void in regions where in-person clinic access has been decimated. Data suggests that approximately one-quarter of all abortions in the United States are now managed via telehealth—a figure that has doubled in the short time since the constitutional right to abortion was revoked.
This shift is backed by a robust body of medical research. Multiple studies, including those published in prestigious medical journals, have consistently demonstrated that medication abortion managed through telehealth is as safe and effective as care provided in a clinical setting.
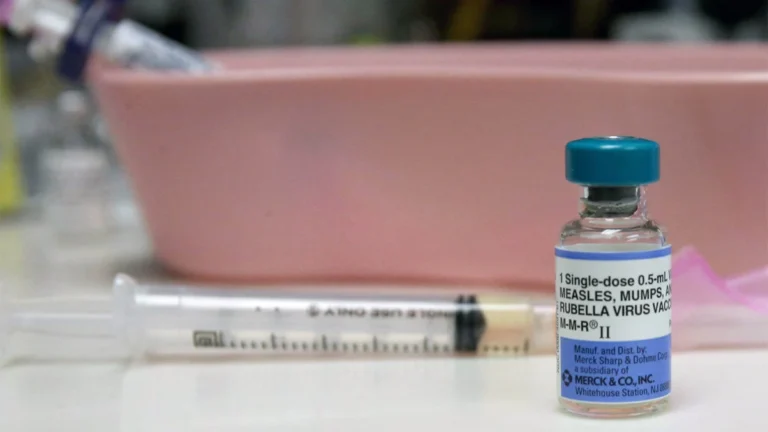
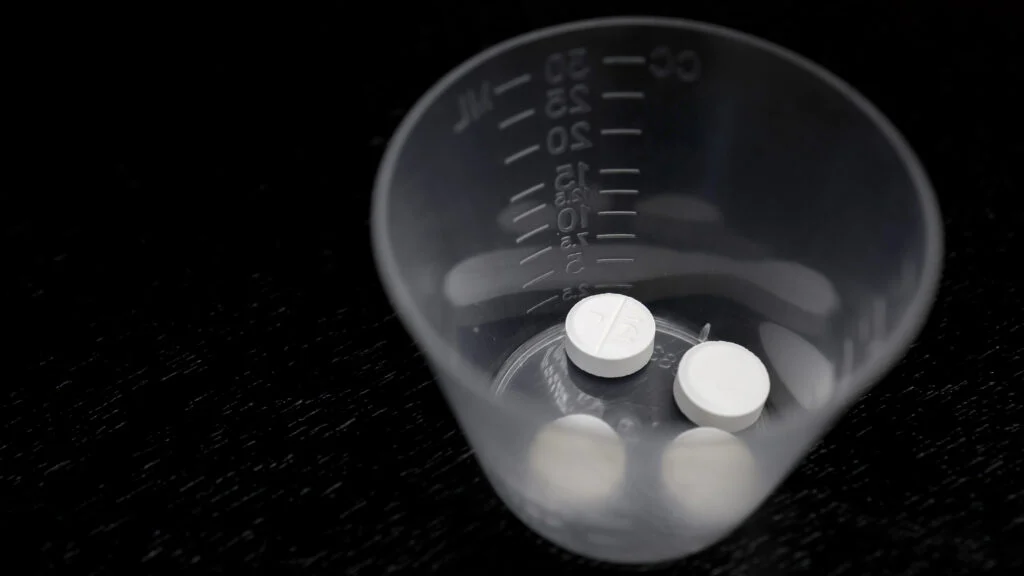
Mifepristone, which works by blocking progesterone—a hormone essential for the development of an embryo—was first approved for medical termination of pregnancy in Europe in the 1980s. While it carries an outstanding safety profile, its U.S. approval was delayed until 2000 due to political, rather than medical, roadblocks. When paired with misoprostol, a prostaglandin that induces uterine contractions, the two-drug regimen allows for a controlled, faster, and more predictable process for patients.
The Professional Obligation: A Physician’s Perspective
From the perspective of those on the front lines of reproductive medicine, the legal effort to restrict mifepristone is not merely a policy dispute; it is a direct interference with the physician’s duty to provide the highest standard of care.
"Doctors have a duty to offer the highest standard of care to our patients," notes Dr. Christine Henneberg, a women’s health physician. "If Louisiana and anti-abortion advocates succeed in further limiting the use of mifepristone, they will be directly interfering with that duty. Instead of ‘saving unborn children,’ they will be causing unnecessary suffering and harm to pregnant women."
The concern among practitioners is that if the two-drug regimen is dismantled, patients will be forced toward less effective, more cumbersome alternatives. While physicians are exploring various pharmacological workarounds, none currently match the efficiency and comfort of the mifepristone-misoprostol combination.
Navigating Potential Alternatives
Should the courts ultimately succeed in restricting mifepristone, the medical community is forced to consider the "misoprostol-only" protocol. Before the introduction of mifepristone, misoprostol was used alone for both miscarriage management and abortion. While effective, it is a harsher experience for the patient. Without mifepristone to "prime" the process, misoprostol requires repeated, higher doses over several days.
The side effects of misoprostol—including intense nausea, vomiting, diarrhea, and flu-like chills—are significant. Furthermore, the rate of incomplete abortions is higher when using misoprostol alone, which increases the likelihood that a patient will require follow-up care or surgical intervention.
Other theoretical alternatives exist, but they are fraught with practical limitations:
- Methotrexate: Used by ER physicians for ectopic pregnancies, this drug is slow-acting. Patients often require weeks to complete the process, and the drug necessitates rigorous laboratory monitoring of liver and kidney function. In the current climate of restricted access, this is not a viable, scalable alternative for telehealth.
- Letrozole: While clinical trials have investigated this breast cancer medication as an alternative, the current regimens require complex dosing schedules—three doses over three days—followed by misoprostol. It lacks the efficiency required for a modern, patient-centered telehealth protocol.
- Ulipristal Acetate: A 2025 study highlighted this emergency contraceptive as a potential alternative. While "proof of concept" results showed efficacy comparable to the two-drug regimen, it remains strictly in the research phase. Experts like Dr. Daniel Grossman of UCSF have warned that even if this drug were to be utilized, the same political forces currently targeting mifepristone would likely pivot to block its use as well.
The Broader Implications for Healthcare
The implications of this legal battle extend far beyond the specific efficacy of one drug. We are witnessing a fundamental shift where the courtroom is increasingly dictating clinical standards. In no other branch of medicine would the judiciary be permitted to override established, FDA-vetted protocols in favor of ideological preferences.
The uncertainty created by this lawsuit places a heavy burden on both providers and patients. Large-volume telehealth providers are already preparing for the possibility of a post-mifepristone landscape, training staff on the nuances of misoprostol-only protocols and bracing for the logistical challenges that would follow.
Ultimately, the goal of those opposing these medications is to create an environment where abortion is as difficult, painful, and inaccessible as possible. Yet, as the medical community has repeatedly emphasized, the desire for bodily autonomy and reproductive control remains constant.
"Regardless of the case’s ultimate outcome, safe and effective medication abortion, including via telehealth, isn’t going away," Dr. Henneberg asserts. "But our most effective regimen still could."
As the Supreme Court weighs the future of reproductive access, the medical community remains in a state of watchful waiting. The core issue remains: whether the practice of medicine should be guided by clinical expertise and patient well-being, or by a series of legal maneuvers designed to force women back into outdated, less efficient, and more traumatic methods of care. Until the final verdict is reached, the status quo remains a fragile, temporary reality, leaving millions of patients in a state of precarious limbo.