By [Your Name/Journalistic Staff]
For millions of women across the United States, the annual or biennial mammogram is a cornerstone of preventative health. Yet, for as routine as the procedure has become, the guidelines governing when and how often a woman should undergo screening remain a landscape of conflicting, and often confusing, medical advice. As major health organizations continue to shift their recommendations, the path toward optimal breast health has become increasingly complex, leaving patients to navigate a maze of disparate protocols.
Main Facts: The Current State of Confusion
The heart of the confusion lies in the disparity between the nation’s leading health authorities. While the American Cancer Society (ACS) has long championed a more aggressive approach, the American College of Physicians (ACP)—a recent entrant into the guideline fray—has taken a more conservative stance.
The fundamental tension rests on the definition of "average risk." Currently, screening guidelines are built upon the assumption that a woman is at average risk and remains asymptomatic. However, breast cancer is a heterogeneous disease; it manifests differently in different women. Consequently, experts are beginning to question the efficacy of a "one-size-fits-all" model.
As it stands, a 42-year-old woman in one state might be told by her primary care physician that she should begin yearly screenings, while a woman of the same age in another jurisdiction might be told to wait until 50. This inconsistency is not a failure of medicine, but rather a reflection of how different groups weigh the benefits of early detection against the potential harms of "over-diagnosis"—the detection of slow-growing tumors that might never have caused clinical problems during a patient’s lifetime.
Chronology: The Evolution of Screening Standards
To understand the current impasse, one must look at how these recommendations have shifted over the last decade.
- Pre-2015: The medical consensus was generally stable, with many groups suggesting annual mammograms beginning at age 40.
- 2015-2020: Several organizations, including the U.S. Preventive Services Task Force (USPSTF), began to move the goalposts, suggesting that the benefits of screening in the 40-49 age bracket were not as clear-cut as once thought, shifting their preference toward starting at age 50.
- 2023-2024: The landscape shifted again. The USPSTF reversed course, recommending that women begin biennial screenings at age 40. However, shortly thereafter, the American College of Physicians issued new, more conservative guidelines, recommending that average-risk women wait until 50 to begin screening every two years.
This "ping-pong" effect in clinical guidance has left both practitioners and patients frustrated. The shifts are often driven by new data regarding the sensitivity of imaging technology and the psychological and physical burden of "false positives," where a mammogram flags a suspicious area that later proves benign, resulting in unnecessary biopsies and extreme patient anxiety.
Supporting Data: Why "Average" is a Misnomer
The primary hurdle in developing universal guidelines is the extreme variability of breast cancer biology. Dr. Laura Esserman, a leading oncology researcher at the University of California, San Francisco, has been a vocal critic of the standardized approach.
"Breast cancer is not one disease," Dr. Esserman emphasizes. "So how in the world does it make sense to screen everybody the same when everyone doesn’t have the same risk?"
The Risk-Benefit Calculus
Data suggests that the frequency of screening should logically correlate with risk. Yet, identifying that risk remains difficult. Aside from the presence of BRCA1 or BRCA2 genetic mutations—which represent only a small fraction of the population—most women lack a clear indicator of their individual risk profile.
- Age as a Proxy: For decades, age has been used as the primary proxy for risk. The incidence of breast cancer rises as women age, which is why older populations have traditionally been the primary target for screening.
- The Burden of Incidence: According to the American Cancer Society, more than 320,000 women will be diagnosed with breast cancer this year in the U.S. While the death rate has steadily declined due to advancements in adjuvant therapies and targeted treatments, the sheer volume of diagnoses makes breast cancer the second-leading cause of cancer death among American women.
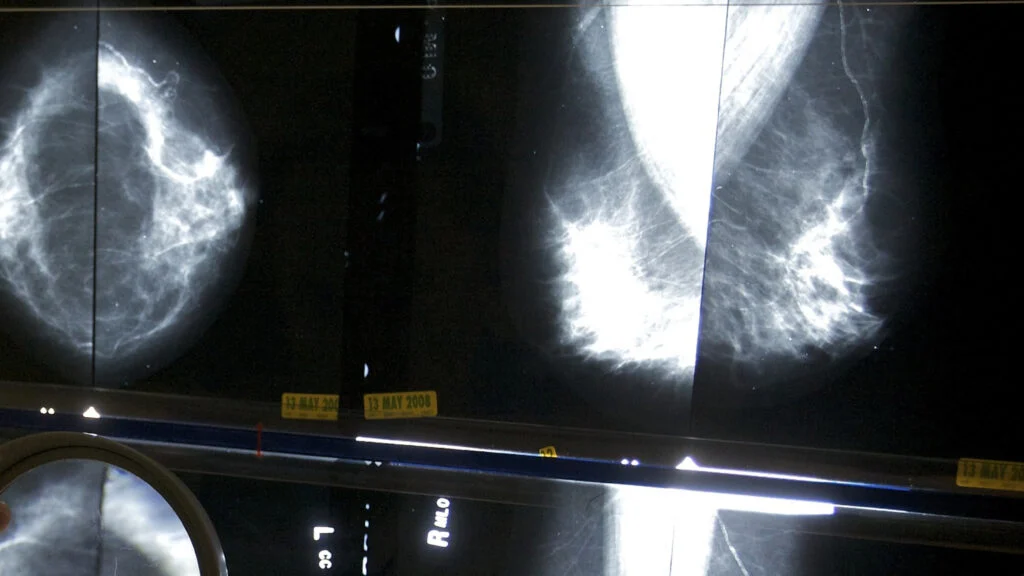
The Problem of Dense Tissue
Approximately 50% of women over the age of 40 have "dense" breast tissue. This presents a technical challenge: dense tissue appears white on a mammogram, and since tumors also appear white, the imaging can effectively hide cancer. While many states now mandate that women be notified of their breast density, the medical community has yet to reach a consensus on whether these women should receive supplemental screening, such as ultrasounds or MRIs, as a standard of care.
Official Responses and Clinical Perspectives
The debate often pits the desire for maximum early detection against the desire for "precision medicine."
Dr. Carolyn Crandall of the University of California, Los Angeles, who chaired the recent ACP report, argues for a more nuanced approach. "We’re not saying there’s no benefit from mammograms in the 40s," she clarifies. "But there’s a narrower balance between the benefits you could get and the harms in 40- to 49-year-olds."
Robert Smith, an expert on early cancer detection for the American Cancer Society, points out that the window of 45 to 49 is a critical period where incidence rates begin to mirror those of women in their early 50s. Consequently, the ACS remains firm in its recommendation that annual screening is appropriate for this demographic.
Furthermore, the disagreement extends to the "stopping point." The American College of Physicians suggests that doctors discuss discontinuing routine screenings for women 75 and older. The American Cancer Society, however, contends that if a woman remains in good health, there is no biological or clinical justification to cease screening, as the risk of breast cancer continues to rise with age.
The Future: Toward Personalized Screening
If the current system is flawed, what does the future hold? The transition toward "risk-based" screening is currently the most promising path forward.
The WISDOM Trial
The WISDOM trial, a study involving nearly 46,000 women, represents a landmark effort to replace age-based guidelines with risk-based ones. By incorporating genetic testing, lifestyle factors, family health history, and breast density, researchers were able to categorize women into specific risk tiers. The study found that a tailored, risk-based approach worked just as effectively as the standard, one-size-fits-all annual screening.
A particularly striking finding from the study was that nearly 30% of women who showed an increased genetic risk had no known family history of the disease. This suggests that relying on family history alone is an insufficient way to assess personal danger.
The Role of Artificial Intelligence
Artificial Intelligence (AI) is also poised to disrupt the status quo. New algorithms are being developed to analyze mammogram images to predict the likelihood of developing cancer in the coming years. By identifying "high-risk" patterns that may be invisible to the human eye, AI could eventually allow radiologists to recommend customized screening intervals for every patient.
Implications for Patients
For the individual woman, the current lack of a unified guideline can feel overwhelming. However, experts suggest that this confusion should not lead to inaction.
- Know Your History: Gather as much information as possible about your family’s cancer history—not just breast cancer, but ovarian and other related cancers.
- Understand Your Biology: Ask your doctor about your breast density after your next mammogram.
- Initiate the Conversation: Given the variance in guidelines, it is incumbent upon the patient to initiate a conversation with their primary care provider or gynecologist about their personal risk profile.
- Consistency is Key: Perhaps the most vital takeaway from public health experts is that screening, regardless of the interval chosen, is most effective when it is consistent.
"Breast screening works best when it’s done regularly," notes Robert Smith. While the medical community continues to refine its stance, the consensus remains that early detection is the single most effective tool in reducing mortality. Until a universal risk-assessment model becomes standard practice, the best strategy for the average woman is to work closely with a trusted physician to create a personalized plan that balances her specific risk factors with her individual preferences for monitoring.
As the field of oncology moves toward a future defined by genomics and AI, the "routine" mammogram may eventually look very different. Until then, the patient remains the most important partner in her own diagnostic journey.