







For the first time since 2018, the medical landscape regarding cardiovascular health has undergone a seismic shift. At the American College of Cardiology’s (ACC) 75th Annual Scientific Session in New Orleans, the ACC and the American Heart Association (AHA) jointly unveiled updated clinical guidance for the screening and management of blood cholesterol. Published simultaneously in the Journal of the American College of Cardiology and Circulation, these recommendations represent the most significant refinement in cardiovascular risk management in nearly a decade.
The updated guidance, titled the 2026 Guideline on the Management of Dyslipidemia, arrives alongside a pivotal paper, "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026," published in the American Journal of Preventive Cardiology. Together, these documents signal a transition from reactive treatment to a proactive, personalized, and lifelong strategy for heart health.
A New Paradigm: Shifting from Reactive to Proactive
The core of the 2026 guidance is a heightened emphasis on lowering low-density lipoprotein (LDL) cholesterol—the "bad" cholesterol—alongside a more granular focus on other atherogenic blood fats, such as lipoprotein(a) or Lp(a).
"We know that lower LDL cholesterol levels are better when it comes to reducing the risk of heart attacks, strokes, and congestive heart failure," says Dr. Roger S. Blumenthal, chair of the guideline writing committee and director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease. "We also know that bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life."
The guidelines argue that waiting until middle age to assess cardiovascular risk is a missed opportunity. By targeting younger demographics and incorporating a broader array of biological markers, clinicians can identify those at risk decades before a catastrophic event occurs.
Chronology: The Path to the 2026 Update
The journey toward these updated standards has been fueled by rapid advancements in genetic research, imaging technology, and pharmacological innovation.
- 2018: The previous landmark guidelines established the foundation for statin therapy and risk stratification.
- 2020–2024: Emerging data from large-scale studies, including the VESALIUS-CV clinical trial, began to suggest that lower cholesterol targets could offer significant protection even for those previously considered low-to-moderate risk.
- March 28, 2026: The formal presentation at the ACC’s 75th Annual Scientific Session in New Orleans, marking the first update in eight years.
- The Future: The 2026 guidance sets the stage for a new era of "precision prevention," where genomic data and longitudinal health tracking will likely become standard components of every physical examination.
Supporting Data: Why Earlier Screening Matters
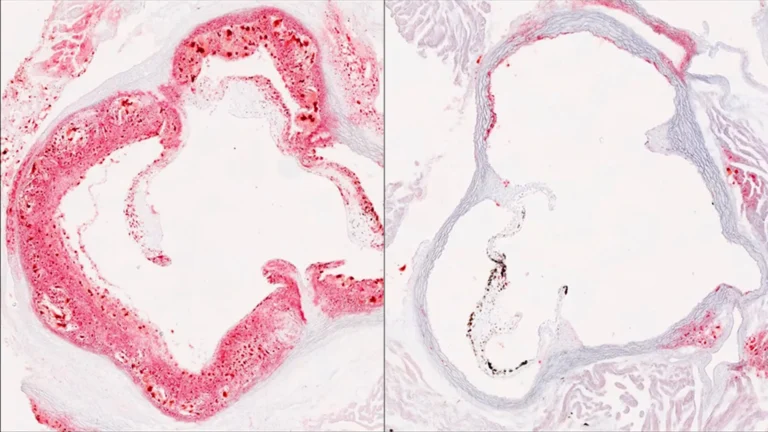
The urgency of these recommendations is underscored by sobering statistics: approximately 1 in 4 adults in the United States currently lives with elevated LDL cholesterol. This condition is the primary driver of atherosclerosis, the silent narrowing and hardening of the arteries that leads to heart disease.
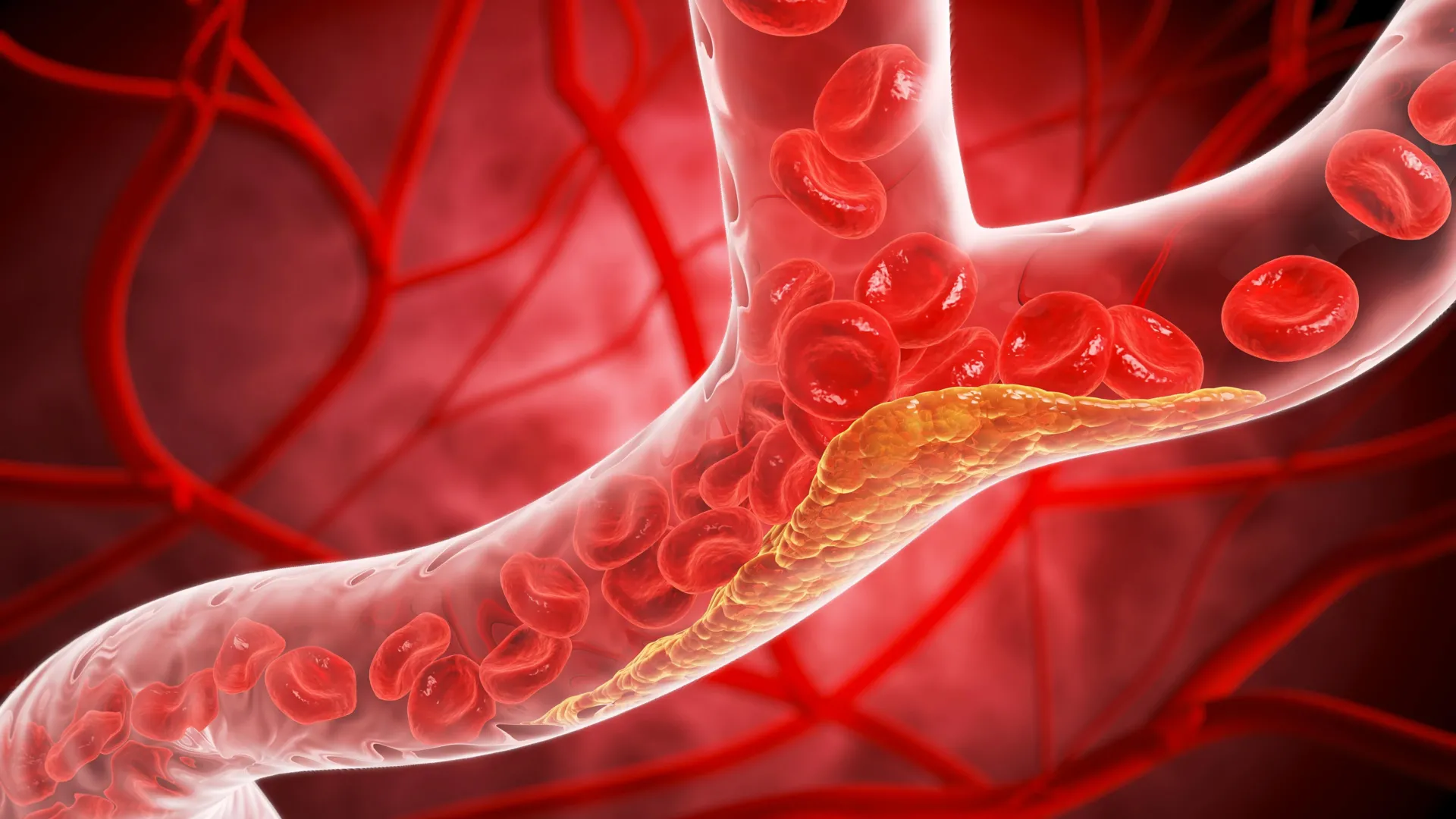
The biological process is insidious. When lipids accumulate within artery walls, they form plaque. This plaque can restrict blood flow, but more dangerously, it can rupture, triggering a sudden heart attack or stroke. The 2026 guidelines posit that by identifying this buildup early—through both traditional screenings and advanced imaging—physicians can intervene before the damage becomes irreversible.
The Role of Genetic Risk
A significant departure from previous guidance is the explicit focus on genetic risk factors. The new guidelines recommend that individuals with familial hypercholesterolemia, a condition characterized by genetically high LDL-C, begin screening as early as age 9.
Furthermore, the guidelines introduce a recommendation for a one-time test for Lipoprotein(a). Elevated levels of Lp(a) are inherited and are strongly correlated with premature heart disease. The data is clear: at levels of 125 nanomoles per liter, risk increases by 40%, and at 250 nanomoles per liter, that risk doubles.
The PREVENT Tool: A Leap Forward in Risk Calculation
Perhaps the most notable technical update is the retirement of the older 10-year risk assessment model in favor of the Predicting Risk of Cardiovascular Disease EVENTs (PREVENT) calculator.
The previous model was limited, focusing primarily on adults over 40 and relying on a narrow set of variables. The PREVENT calculator, however, is a massive upgrade:
- Broader Data Pool: Based on data from 6.6 million individuals, compared to the 26,000 used for previous models.
- Expanded Metrics: Includes blood sugar and kidney function, providing a more holistic view of systemic health.
- Earlier Intervention: Designed for use starting at age 30, allowing for a 30-year risk projection rather than just a 10-year outlook.
"Shifting the paradigm toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease and lead to better health outcomes for people decades later," explains Dr. Seth Martin, a cardiologist and member of the writing committee.
Clinical Implications and "Risk Enhancers"
For patients who fall into the "borderline" or "moderate" risk categories, the guidelines introduce the concept of "risk enhancers." These are clinical indicators that allow doctors to decide if a patient needs more aggressive therapy.
These enhancers include:
- Inflammatory Markers: Measuring high-sensitivity C-reactive protein (hsCRP).
- Family History and Ancestry: Acknowledging that genetics play a significant role in individual risk profiles.
- Advanced Imaging: Coronary artery calcium scans are now more strongly encouraged to visualize actual plaque buildup in the heart’s vessels.
- Life Events: For women, the guidelines specifically call for the consideration of pregnancy-related complications, such as preeclampsia and gestational diabetes, as significant markers of future cardiovascular risk.
Expanded Treatment Options and Aggressive Targets
The 2026 guidelines do not just change how we identify risk; they change how we manage it. While statins remain the cornerstone of therapy, the new guidelines provide a clear roadmap for using non-statin therapies—including ezetimibe, bempedoic acid, and PCSK9 monoclonal antibodies—to reach target levels.
The New Target Tiers:
- Low-to-Intermediate Risk: LDL-C should be kept below 100 mg/dL.
- Intermediate Risk: The target is reduced to below 70 mg/dL.
- High Risk: The target is now below 55 mg/dL.
These targets also extend to non-HDL cholesterol and apolipoprotein B, reflecting a modern understanding that cholesterol management is about more than just one specific lipid measurement.
Official Responses and Future Outlook
The release has been met with broad support from the cardiology community, though it places a new demand on primary care physicians to integrate these complex, personalized risk assessments into their daily practice.
In an accompanying editorial, experts noted that the guidance might be even more aggressive in the future. The VESALIUS-CV trial findings suggest that for individuals with moderate atherosclerosis, pushing LDL-C even lower than 55 mg/dL may yield significant, long-term survival benefits.
Despite these advanced medical interventions, the guidelines emphasize that the foundation of heart health remains unchanged: a balanced diet, consistent physical activity, tobacco cessation, adequate sleep, and weight management. According to Dr. Blumenthal, 80% to 90% of cardiovascular disease is linked to modifiable lifestyle factors. The 2026 guidelines are not a replacement for these habits, but rather a sophisticated, data-driven safety net designed to protect patients when lifestyle changes alone are not enough.
As healthcare moves toward this more personalized, data-rich era, the message from the ACC and AHA is clear: by combining the best of modern technology with a focus on early, lifetime prevention, we can fundamentally redefine the human experience of aging and heart health.