







In the landscape of modern cardiology, the "risk score" has long served as the primary compass for physicians. Tools like the ASCVD (Atherosclerotic Cardiovascular Disease) risk calculator and the newer PREVENT tool are the standard gatekeepers for preventative care, determining which patients receive life-saving interventions like statins. However, a groundbreaking study led by researchers at the Icahn School of Medicine at Mount Sinai has cast a shadow of doubt over these widely accepted practices, suggesting that current screening methods are failing to identify nearly half of those at risk for a heart attack.
The findings, published on November 21 in the Journal of the American College of Cardiology: Advances, suggest that the current paradigm—which relies on population-based risk scores and the onset of symptoms—may be fundamentally flawed, leaving millions of individuals dangerously exposed to cardiac events that are currently considered "unpredictable" by standard metrics.
The Myth of the "Low-Risk" Patient
For decades, the medical community has utilized risk calculators to estimate the likelihood of a cardiovascular event within a 10-year window. These tools weigh factors such as age, sex, race, blood pressure, cholesterol levels, diabetes status, and smoking history. The logic is simple: if a patient falls into the "low" or "borderline" risk category and reports no symptoms like chest pain or shortness of breath, they are often sent home with a clean bill of health.
However, the Mount Sinai study, which conducted a retrospective analysis of 474 patients who suffered their first heart attack, revealed a chilling reality. If those same patients had been assessed just 48 hours before their cardiac events, nearly half would have been categorized as low or borderline risk by the ASCVD tool. Even more concerning, the newer PREVENT tool—designed to be a more comprehensive evolution of cardiovascular risk assessment—would have categorized over 60 percent of those patients as low or borderline risk.
"Our research shows that population-based risk tools often fail to reflect the true risk for many individual patients," explains Dr. Amir Ahmadi, the study’s corresponding author and a Clinical Associate Professor of Medicine (Cardiology) at Mount Sinai. "If we had seen these patients just two days before their heart attack, nearly half would not have been recommended for further testing or preventive therapy guided by current risk estimate scores and guidelines."
Chronology of a Crisis: Why Symptoms Arrive Too Late
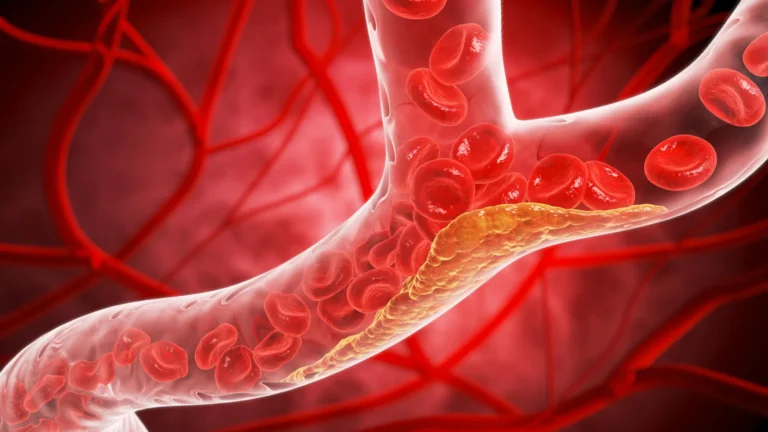
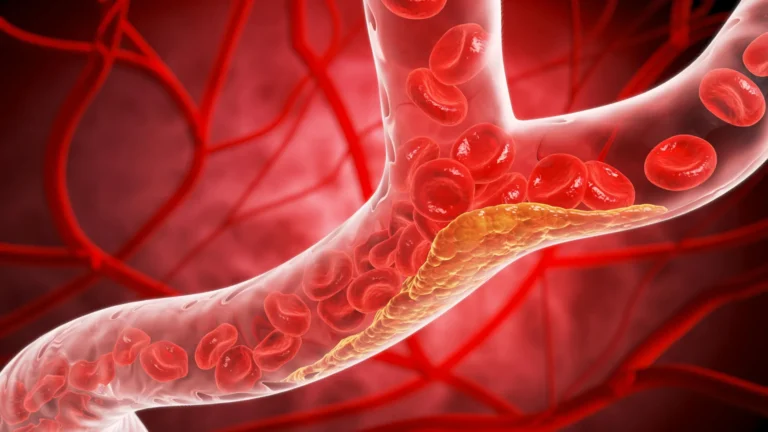
The study’s findings highlight a dangerous mismatch between the medical definition of "at risk" and the biological reality of atherosclerosis. Atherosclerosis, the buildup of fats and cholesterol in the artery walls, is a slow, silent process. It can progress for years without causing the classic symptoms that doctors are trained to look for.
The researchers found that for 60 percent of the study participants, physical symptoms such as chest pain or shortness of breath did not emerge until fewer than two days before the heart attack. This timeline is critical: it suggests that by the time a patient presents with symptoms, the underlying pathology has already reached a critical stage where a rupture is imminent.
The medical model currently relies on these symptoms as "gatekeepers." If a patient is asymptomatic and has a low risk score, they are rarely offered advanced diagnostic imaging. The Mount Sinai data suggests that this approach is reactive rather than proactive. By waiting for a "high-risk" score or the onset of symptoms, the medical system is effectively waiting for the disease to reach its final, most dangerous phase before intervening.
Data Breakdown: A Failure of Predictive Modeling
The study focused on 474 patients under the age of 66 who had no known history of coronary artery disease. All patients were treated for their first heart attack at either Mount Sinai Morningside or The Mount Sinai Hospital between January 2020 and July 2025.
To determine the efficacy of current screening, investigators performed a simulation. They gathered comprehensive data on each patient—including demographics, medical history, and clinical markers—and calculated their 10-year ASCVD risk score as it would have appeared two days before their cardiac event.
The Findings at a Glance:
- ASCVD Failure Rate: 45 percent of patients who suffered a heart attack would not have qualified for preventive therapy under current guidelines.
- PREVENT Failure Rate: 61 percent of those patients would have been categorized as low or borderline risk, missing the opportunity for intervention.
- The Symptom Gap: 60 percent of patients experienced symptoms less than 48 hours before their event, proving that symptom-based diagnosis is often synonymous with emergency-level intervention rather than prevention.
These figures illustrate that the tools, while useful for managing large population health trends, are remarkably poor at capturing the nuances of individual pathology. A patient can have "perfect" blood pressure and "normal" cholesterol and still harbor unstable, rupture-prone plaque in their coronary arteries.
Official Perspectives: Shifting the Paradigm
The implications of this study are profound, suggesting a need to shift the focus from "risk estimation" to "direct visualization."
"This study suggests that the current approach of relying on risk scores and symptoms as primary gatekeepers for prevention is not optimal," Dr. Ahmadi notes. "It may be time to fundamentally reconsider this model and move toward atherosclerosis imaging to identify the silent plaque—early atherosclerosis—before it has a chance to rupture."
Dr. Anna Mueller, the study’s first author and an internal medicine resident at Icahn Mount Sinai, emphasizes that the reliance on these scores provides a false sense of security. "When we look at heart attacks and trace them backwards, most heart attacks occur in patients in the low or intermediate risk groups," she explains. "This study highlights that a lower risk score, along with not having classic heart attack symptoms, is no guarantee of safety on an individual level."
The researchers argue that the medical field must move toward a model where patients with potential markers for plaque—even those deemed "low risk"—are offered non-invasive imaging. By identifying "silent" plaque, physicians could initiate aggressive lipid-lowering therapies or lifestyle interventions years before a life-threatening event occurs.
Implications for Future Cardiology
The study serves as a wake-up call for primary care physicians and cardiologists alike. If the tools currently used to guide the prescription of statins and other cardiac medications are missing over half of the people who go on to have heart attacks, the current healthcare model is inadvertently allowing a massive number of preventable events to occur.
The Path Forward:
- Re-evaluating Guidelines: Medical boards may need to reconsider the reliance on ASCVD and PREVENT scores as the sole criteria for determining which patients receive advanced screening.
- The Rise of Imaging: Incorporating coronary artery calcium (CAC) scoring or other advanced imaging techniques could provide a more accurate picture of individual danger than a simple mathematical formula.
- Personalized Risk Assessment: There is a pressing need for a move toward personalized medicine, where individual arterial health is measured directly rather than estimated through population averages.
While the researchers acknowledge that more work is required to refine these diagnostic shifts, the message is clear: the current "wait-and-see" approach, dictated by risk scores and the emergence of symptoms, is insufficient. By moving the goalposts from risk estimation to the detection of silent disease, the medical community could potentially save countless lives, turning what is currently a "silent killer" into a manageable and treatable condition.
As the study concludes, the challenge now lies in translating these findings into clinical practice. For the millions of patients currently categorized as "low risk," this study offers both a warning and a potential road to better, earlier care. The future of cardiology, it seems, lies not in the numbers on a calculator, but in the clarity of an image.