







For decades, the standard barometer for heart health in America has been the LDL cholesterol test. Millions of patients annually sit in exam rooms, awaiting the results of their lipid panels, bracing for a number that dictates whether they will be prescribed statins or advised to adjust their diet. However, a landmark study from Northwestern Medicine suggests that our reliance on traditional LDL measurements may be leaving millions of patients under-treated and at preventable risk.
New research, published in the journal JAMA, indicates that measuring apolipoprotein B (apoB) is a significantly more effective method for identifying patients who require aggressive cholesterol-lowering therapy. By shifting the clinical focus from the weight of cholesterol to the count of harmful particles, medical professionals could theoretically prevent a massive surge of heart attacks and strokes across the United States.
The Science of the "Particle Count"
To understand why the medical community is buzzing about apoB, one must first understand the limitations of the current standard. Traditional LDL (low-density lipoprotein) testing measures the total concentration of cholesterol carried by particles in the blood. Non-HDL cholesterol, another common metric, attempts to cast a wider net by including all "bad" cholesterol types.
While these metrics have served as the bedrock of cardiology for years, they are fundamentally indirect. They measure the mass of cholesterol rather than the actual number of culprit particles.
"We found that apoB testing to intensify cholesterol-lowering medication would prevent more heart attacks and strokes than current practice," says Dr. Ciaran Kohli-Lynch, the study’s lead author and an assistant professor of preventive medicine at Northwestern University Feinberg School of Medicine. "Research strongly shows that apoB is better at identifying who is at risk, because it counts the total number of harmful particles in the blood."
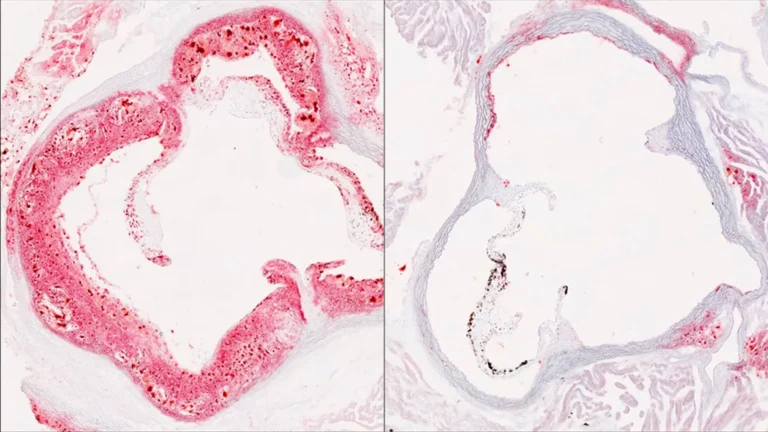
These tiny particles, known as atherogenic lipoproteins, are the silent architects of cardiovascular disease. Over time, they infiltrate the walls of the arteries, where they oxidize and transform into plaques. These plaques restrict blood flow and, if they rupture, trigger the catastrophic events—heart attacks and strokes—that remain the leading cause of death in the United States. By counting the particles themselves, rather than the cholesterol they carry, clinicians get a much higher-resolution map of a patient’s actual risk profile.
A Chronology of Cardiovascular Risk Assessment
The evolution of cholesterol testing has been a slow, incremental process. For the better part of the late 20th century, total cholesterol was the only metric that mattered. As lipidology matured, doctors began distinguishing between "good" (HDL) and "bad" (LDL) cholesterol, leading to the refinement of the lipid panel most patients recognize today.
However, the "LDL era" has increasingly come under fire as researchers realized that patients with "normal" LDL levels were still suffering from heart attacks.
- The Early Era (1970s–1990s): Focus on total cholesterol. High levels were linked to heart disease, but the nuance of particle size and density was poorly understood.
- The Refinement Era (2000s–2015): The medical community standardized LDL and non-HDL cholesterol as the primary targets for statin therapy. Guidelines became more rigid, leading to widespread statin usage.
- The Precision Era (2016–Present): With the advent of advanced lipidomics, researchers began advocating for apoB. The argument was simple: every single harmful particle contains exactly one molecule of apoB. Therefore, apoB is a perfect "particle counter."
The current study from Northwestern marks a turning point, as it is the first comprehensive analysis to demonstrate not just the clinical superiority of apoB, but its economic viability.
Modeling the Future of Preventative Care
To test the efficacy of this shift, the Northwestern research team—which included Dr. John Wilkins and Dr. Samuel Luebbe—constructed a sophisticated computer simulation. They modeled a representative cohort of 250,000 U.S. adults who were eligible for statin therapy but had not yet developed cardiovascular disease.
The simulation compared three distinct strategies for guiding treatment:
- The LDL Approach: Treating based on traditional low-density lipoprotein levels.
- The Non-HDL Approach: Treating based on the broader spectrum of harmful cholesterol.
- The ApoB Approach: Using the particle count to dictate when to intensify therapy.
When patients failed to reach their target levels under these models, the simulation moved them to more aggressive interventions, including higher-dosage statins and the addition of ezetimibe. The researchers tracked these cohorts over a lifetime, measuring life expectancy, quality of life, the number of cardiovascular events, and total healthcare expenditure.
The results were striking: the apoB-guided strategy consistently outperformed the others. By identifying patients whose high particle counts were masked by "normal" cholesterol levels, the apoB method prevented more heart attacks and strokes. Critically, the study found that these health improvements were achieved at a cost that represents "good value" for the U.S. healthcare system.
The Economic and Clinical Implications
One of the primary hurdles to the widespread adoption of apoB testing has been cost and convenience. Historically, it has required an additional blood draw, separate from the standard lipid panel. Many healthcare systems have been hesitant to mandate a test that adds administrative and financial burdens to routine check-ups.
"Our study asked: Is it worth spending extra money to use apoB instead of LDL to guide treatment intensification?" Dr. Kohli-Lynch noted. The answer, according to the simulation, is a resounding yes. The downstream savings—gained by preventing expensive emergency room visits, hospitalizations, surgeries, and long-term disability—far outweigh the incremental cost of the blood test itself.
This study arrives at a critical juncture. Earlier this year, the American Heart Association (AHA) and ten other major medical organizations released updated guidelines that recommend younger patients begin cholesterol-lowering therapy sooner than previously suggested. As the pool of people on statins grows, the need for precision becomes paramount.
"This means it is increasingly important to accurately identify who would benefit most from intensive treatment," says Kohli-Lynch. If we are to start treating younger, healthier people, we must be certain we are treating the right ones. Over-treating the low-risk population is an unnecessary financial burden, while under-treating those with high particle counts is a public health failure.
Official Responses and The Path Forward
The medical community has greeted the study with significant interest. While the AHA and other bodies have not yet mandated a wholesale shift to apoB as the primary clinical standard, the study provides the necessary evidence-based justification for such a policy change.
For the patient, the implications are profound. If your doctor currently relies solely on an LDL test, you may be missing a critical piece of your health puzzle. The move toward apoB represents a shift toward "precision cardiology"—a world where your treatment plan is based on your unique biological makeup rather than generic population averages.
Summary of Key Findings
- ApoB is a direct measure: It tracks the actual number of dangerous particles, rather than the total weight of the cholesterol within them.
- Improved Outcomes: The simulation confirmed that apoB-guided care leads to fewer heart attacks and strokes over a lifetime.
- Cost-Effectiveness: Despite the added cost of the test, the long-term economic benefits to the healthcare system are substantial.
- Clinical Urgency: With new guidelines pushing for earlier intervention, the accuracy of risk assessment is more important than it has ever been.
As the findings from this Northwestern study circulate through medical boards and policy committees, the conversation around the standard lipid panel is likely to change. The era of the "one-size-fits-all" cholesterol test may be drawing to a close, replaced by a more nuanced, precise, and ultimately safer approach to heart health. For the millions of Americans managing their cardiovascular risk, the future looks more accurate—and for many, that accuracy could mean the difference between a lifetime of health and a life-altering medical emergency.