









For the first time since 2018, the American College of Cardiology (ACC) and the American Heart Association (AHA) have issued a comprehensive update to clinical guidance on the screening and management of blood cholesterol. Unveiled on March 28 at the ACC’s 75th Annual Scientific Session in New Orleans, these guidelines represent a fundamental shift in how medicine approaches the prevention of cardiovascular disease (CVD). Published simultaneously in the Journal of the American College of Cardiology and Circulation, the updated recommendations move away from a "one-size-fits-all" approach, championing a more granular, personalized, and early-intervention strategy.
The Evolution of Cardiovascular Care: A Chronological Context
The 2026 guidelines arrive at a critical juncture in public health. While the 2018 recommendations provided a robust framework for managing lipids, the landscape of cardiovascular science has evolved rapidly in the last eight years.
- 2018: The previous iteration of the guidelines established the standard for statin therapy and introduced risk-based stratification.
- 2023–2025: A wave of clinical trials, including data from the VESALIUS-CV study, began to suggest that lower LDL-C targets—previously considered aggressive—offered significant protective benefits. Simultaneously, the integration of big data and advanced genetic testing began to highlight the limitations of older risk-prediction models.
- March 2026: The official release of the new guidance marks the first major update in nearly a decade, incorporating advancements in precision medicine and long-term risk prediction.
- Post-Release: Shortly following the announcement, the American Journal of Preventive Cardiology published a supplemental paper titled, "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026," reinforcing the necessity of translating these complex clinical shifts into actionable patient communication.
The Core Philosophy: Personalization and Aggressive Targets
At the heart of the 2026 guidance is the principle that lower LDL cholesterol (LDL-C)—often termed "bad cholesterol"—is unequivocally superior for long-term vascular health. However, the new document goes beyond merely recommending lower numbers; it advocates for a shift in the timing of interventions.
"We know that lower LDL cholesterol levels are better when it comes to reducing the risk of heart attacks, strokes, and congestive heart failure," says Dr. Roger S. Blumenthal, chair of the guideline writing committee and director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease. "We also know that bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life."
The New Lipid Targets
The guidelines categorize patients by risk, with increasingly stringent goals:
- Low-to-Moderate Risk: LDL-C levels should ideally remain below 100 mg/dL.
- Intermediate Risk: Clinicians are advised to target levels below 70 mg/dL.
- High Risk: The target is now set at less than 55 mg/dL.
Furthermore, the guidelines have expanded to include specific targets for non-HDL cholesterol and apolipoprotein B, providing clinicians with a more comprehensive "lipid panel" to monitor.
Addressing the Silent Threat: Why Earlier Screening Matters
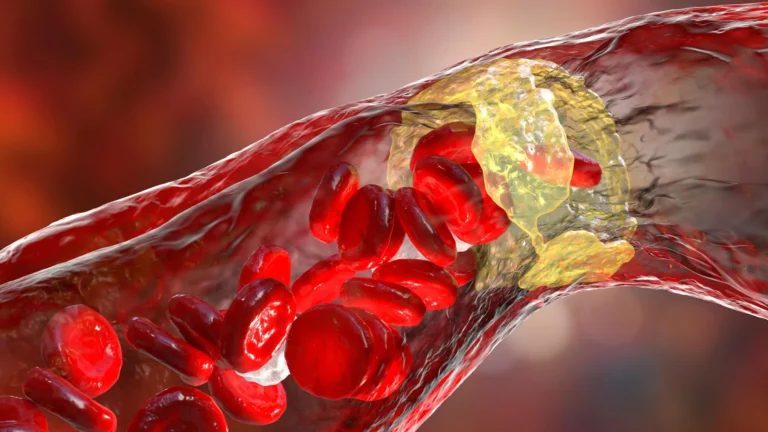
Roughly one in four American adults currently lives with elevated LDL-C, a primary driver of atherosclerosis—the hardening and narrowing of arteries. When lipid particles accumulate, they form plaques that not only restrict blood flow but pose the risk of sudden rupture, which often serves as the trigger for a heart attack or stroke.
The new guidance emphasizes that waiting for middle age to address cholesterol is a missed opportunity. Because atherosclerosis is a cumulative process, the committee is urging clinicians to identify risk factors earlier. This includes a more rigorous screening process for familial hypercholesterolemia, with genetic or lipid screening now recommended for children as young as nine.
The Role of Genetic Risk: Lp(a)
For the first time, the guidelines place significant weight on lipoprotein(a), or Lp(a). This genetically determined particle is an independent risk factor for heart disease. The new recommendation is for a one-time screening for Lp(a) levels. Data indicates that levels of 125 nmol/L can increase heart disease risk by 40%, while levels reaching 250 nmol/L can double that risk. By identifying these individuals early, clinicians can initiate more proactive, lifelong management strategies.
The PREVENT Calculator: A Technological Leap
Perhaps the most transformative aspect of the 2026 update is the introduction of the "Predicting Risk of Cardiovascular Disease EVENTs" (PREVENT) calculator.
The previous risk-assessment model was limited: it focused primarily on 10-year risk for patients aged 40 and older, using a narrow set of variables. The PREVENT tool, however, is a massive leap forward. Built on longitudinal data from 6.6 million individuals—a stark contrast to the 26,000 used in previous models—the PREVENT calculator allows for:
- Earlier Prediction: It is designed for use starting at age 30.
- Expanded Scope: It integrates critical health markers such as kidney function and blood sugar levels, providing a more holistic view of systemic risk.
- Long-Term Vision: It offers both 10-year and 30-year projections, helping patients and doctors understand the "life course" trajectory of their cardiovascular health.
"Shifting the paradigm toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease and lead to better health outcomes for people decades later," notes Dr. Seth Martin, a member of the guideline writing committee.
Beyond the Numbers: "Risk Enhancers" and Lifestyle
While pharmacology is a cornerstone of the new guidance, the committee remains steadfast that the foundation of heart health is lifestyle. Dr. Blumenthal estimates that 80% to 90% of cardiovascular disease is linked to modifiable factors. The guidance reinforces the "Big Five": a balanced, nutrient-dense diet, consistent physical activity, tobacco cessation, adequate sleep, and weight management.
However, for patients in the "borderline" or "moderate" risk categories, the guidelines introduce "risk enhancers" to help break ties on treatment decisions. These include:
- Inflammation Markers: Use of high-sensitivity C-reactive protein (hsCRP) testing.
- Imaging: Utilizing coronary artery calcium scans to visually confirm the presence of plaque.
- Clinical History: Factoring in systemic conditions like rheumatoid arthritis, as well as specific life events such as preeclampsia, gestational diabetes, or early menopause, which are now recognized as critical indicators of future cardiovascular risk in women.
Expanded Treatment Options
The 2026 guidelines acknowledge that statins, while effective, are not sufficient for every patient. The document provides updated protocols for using non-statin therapies, including ezetimibe, bempedoic acid, and PCSK9 monoclonal antibodies. These therapies are highlighted as essential tools for patients who are statin-intolerant or those whose LDL-C levels remain stubbornly high despite standard therapy.
Importantly, the guidelines provide specific clinical pathways for traditionally underserved or complex populations, including those with advanced kidney disease, HIV, cancer, or those who are pregnant or breastfeeding. By tailoring treatment to these specific physiological profiles, the guidelines aim to ensure that no patient is left behind due to the complexity of their underlying health status.
Implications for the Future of Cardiology
The publication of these guidelines is not merely an academic exercise; it is a call to action for the medical community to embrace a more proactive, data-driven, and personalized model of care. The inclusion of the VESALIUS-CV trial findings in the supporting literature suggests that the ceiling for "optimal" cholesterol levels may continue to drop.
As medical technology advances, the ability to detect plaque earlier through imaging and to predict events decades in advance through the PREVENT calculator will fundamentally change the patient-doctor relationship. No longer will the conversation be centered on "reacting" to a heart attack or high blood pressure reading. Instead, the focus has shifted to "preventive maintenance" of the vascular system.
The 2026 Guideline on the Management of Dyslipidemia stands as a testament to the progress of modern cardiology. By fostering shared decision-making between patients and clinicians, and by grounding treatment in the most robust data set in the history of the field, the ACC and AHA have set a new standard for how we define, monitor, and protect the human heart. The era of precision cardiovascular prevention has arrived, and it promises to reshape the longevity and quality of life for millions.