











For years, I found myself unable to utter the phrase, "my ostomy bag saved my life." It felt like a claim reserved for those with clear-cut pathology—those battling inflammatory bowel disease (IBD), acute infections like diverticulitis, or the undeniable presence of a tumor. In those cases, the medical consensus is often binary: there is a visible threat, and the surgical intervention is the clear solution.
My reality, however, was anchored in the murky, less measurable waters of Ehlers-Danlos syndrome (EDS). My gastrointestinal (GI) dysfunction was not a textbook case; it was a multisystemic, structural nightmare that left many medical providers stumped. Today, two years post-surgery, I am sharing my story not just to celebrate a milestone, but to provide a roadmap for the patients who feel unseen and the providers who need a new lens through which to view chronic, treatment-resistant GI failure.
Understanding the Surgical Intervention: What is an Ostomy?
An ostomy is a life-altering surgical procedure that creates an opening, known as a stoma, in the abdominal wall. This allows waste to bypass the traditional route—the rectum—and exit the body into an external pouch.
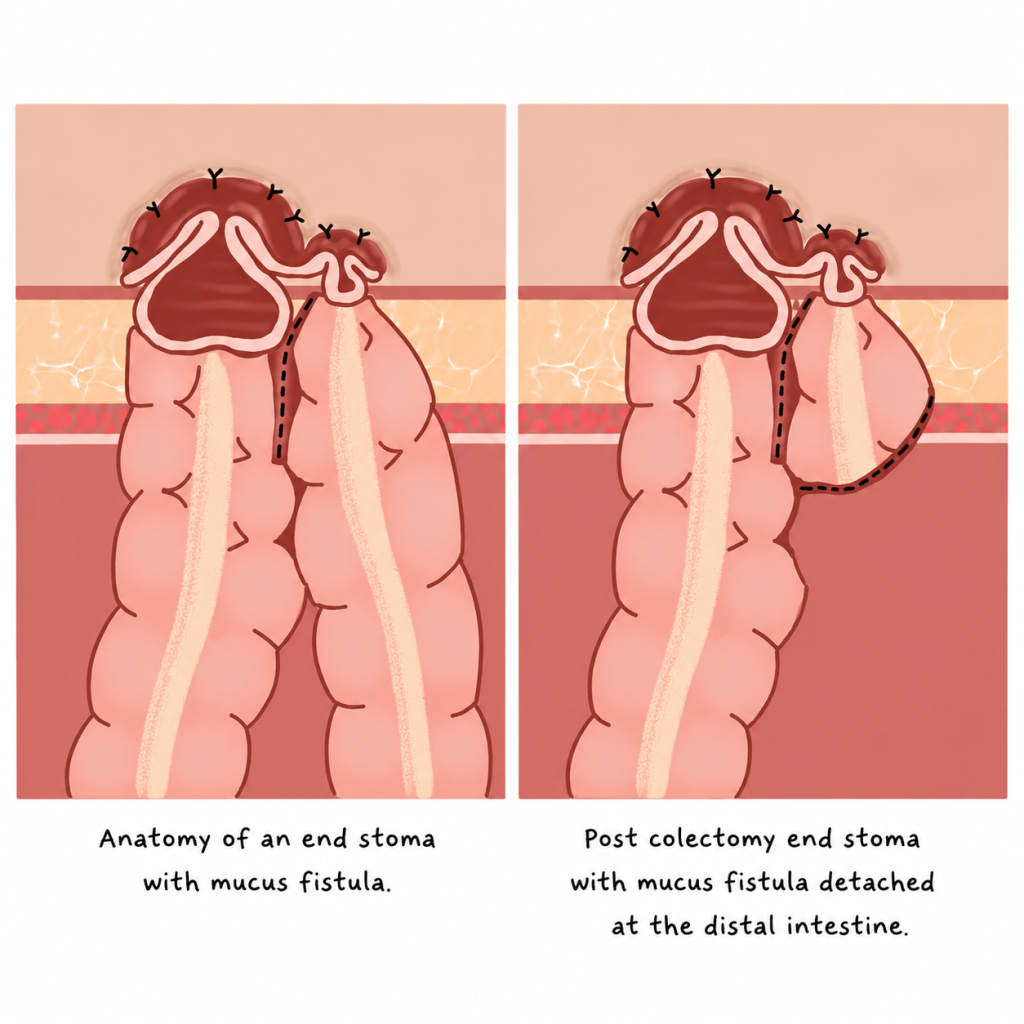
While the concept is straightforward, the execution varies. I live with a permanent end ileostomy, a procedure where the small intestine is brought to the surface of the abdomen. My colon was subsequently removed. This differs from a loop ostomy, which is often temporary, where a loop of bowel is exteriorized. In my specific case, the large intestine remained in the body for a period alongside the end stoma, sometimes referred to as an end-stoma with a mucus fistula, allowing for a phased transition.
The EDS Connection: A Lifetime of "Just Constipation"
Ehlers-Danlos syndrome is a collection of connective tissue disorders. Because connective tissue acts as the biological scaffolding for our entire body, its dysfunction is inherently multisystemic. It affects blood vessels, joints, skin, and—crucially—the organs. For me, EDS manifested as a total breakdown of my gastrointestinal tract.
The Chronology of Chronic Dysfunction
My struggle did not begin in adulthood; it was the backdrop of my entire life.
- Childhood: I recall the hallways of elementary school, doubled over in pain, waiting for a wave of agony to subside.
- Adolescence: Middle school became a gauntlet of bathroom visits that yielded no results. I learned to mask my suffering with humor, a common coping mechanism for children with chronic, invisible illnesses.
- Early Adulthood: By college, the "embarrassing" symptoms had escalated into a debilitating reality. I was housebound, terrified of the unpredictable nature of my own digestion.
I exhausted every conventional recommendation: high-fiber diets, aggressive laxative regimens, motility stimulants, and pelvic floor physical therapy. None provided relief. My symptoms were not merely "constipation"—they were a systemic obstruction of life.

The Road to Diagnosis: Navigating the Medical Labyrinth
When a GI specialist finally moved beyond dismissing my symptoms as "just constipation," a long-overdue investigation began. This was not a linear path; it was a crusade of advocacy.
The Cascade of Diagnostic Testing
To reach a diagnosis, I underwent a rigorous series of tests, including:
- Sitz Marker Studies: To measure the speed of colonic transit.
- Defecography: To visualize the mechanics of bowel movements under X-ray.
- Manometry: To assess the pressure and nerve function of the rectum and anus.
- Advanced Imaging: Including specialized scans to identify visceroptosis—the abnormal downward displacement of organs.
Throughout this process, I frequently found myself in the role of educator, providing radiologists and surgeons with current research on how connective tissue disorders mimic and exacerbate functional GI disorders.
What the testing revealed: The results confirmed a profound structural and functional failure. My organs were not sitting where they belonged, and my bowel was incapable of the rhythmic contractions required for waste elimination. It wasn’t "functional" in the sense of being "all in my head"—it was a mechanical, physical failure of the body’s support structures.
The Decision: Overcoming the Fear of the Unknown
When my colorectal surgeon first used the word "permanent," I experienced a moment of existential whiplash. The prospect of an ostomy brings a host of valid anxieties:
- Physicality: Will it leak? Will it be visible under clothes?
- Social: How does this impact intimacy and attraction?
- Psychological: Will my contamination OCD spiral out of control?
- Existential: What if the surgery fails to fix the pain?
I spent months in a cycle of self-gaslighting, questioning if I was "sick enough" to warrant such a radical intervention. But when I looked at my current existence—the pain, the isolation, the loss of autonomy—the fear of the bag faded compared to the reality of staying the same.
Surgical Reality: Recovery and the Path to Thriving
My first surgery to create the stoma provided immediate, visceral relief. The heaviness and bloating that had plagued me for decades began to dissipate. A year later, I underwent a total colectomy—a ten-hour procedure to remove over seven feet of colon that had become, effectively, dead weight.
The recovery was, as any EDS patient would expect, non-linear. Healing with connective tissue fragility is a marathon, not a sprint. I had to advocate for myself from the hospital bed, ensuring my surgical team understood the unique challenges of my physiology. Despite the bumps in the road, the outcome was undeniable: the moment my stoma was functional, my body felt fundamentally different.
Implications: Living Beyond the Stoma
Today, I have reclaimed my life. I have even channeled my experience into a small business, sewing custom ostomy bag covers to provide others with the confidence I had to fight to find. My platform has allowed me to advocate on a global stage, including traveling to Kenya with Campaign 52 to provide resources to women in underserved regions.
A Message to Patients
If you are an EDS patient with unexplained, treatment-resistant GI symptoms, please hear this: You are not imagining it. The fact that your symptoms are not "measurable" by standard metrics does not make them any less excruciating. Do not stop seeking answers until you find a provider who understands the link between connective tissue and GI motility.
A Message to Providers
When an EDS patient presents with a lifetime of GI dysfunction, please set aside the assumption that the symptoms are psychosomatic. Investigate the structural, the "rare," and the systemic. Your patients are not exaggerating; they are often the most accurate reporters of their own failing biology.
A Final Thought on Grief and Hope
Living with an ostomy is not without its hardships. Leaks occur. Skin irritation happens. There is a grieving process for the body you once had. But on the other side of that grief is a life of freedom. I am two years into this journey, and I can say with total conviction: the bag did not take my life away—it gave it back.
Disclaimer: The experiences described in this article are those of the author and may not reflect the experiences of all people with EDS, gastrointestinal dysmotility, or ostomies. This content is for educational purposes only and does not constitute medical advice. Please consult your healthcare team regarding your individual medical circumstances.







