KAMPALA, Uganda — In a move that defies international health guidance but underscores the growing desperation to contain a deadly contagion, Ugandan authorities have ordered an immediate closure of the nation’s border with the Democratic Republic of the Congo (DRC). The decision comes as health officials scramble to track a surge of the Bundibugyo strain of the Ebola virus, an exceptionally dangerous and rare variant for which no approved vaccines or specific therapeutics currently exist.
The closure, announced by Dr. Diana Atwine of the Ugandan Ministry of Health, serves as a stark acknowledgment that the regional containment strategy is faltering. With Ugandan health workers already exposed to the virus via patients who crossed the border before the outbreak was officially declared on May 15, the risk of a domestic epidemic has transitioned from a theoretical concern to an urgent national security priority.
The Core Facts: A Pathogen Without a Cure
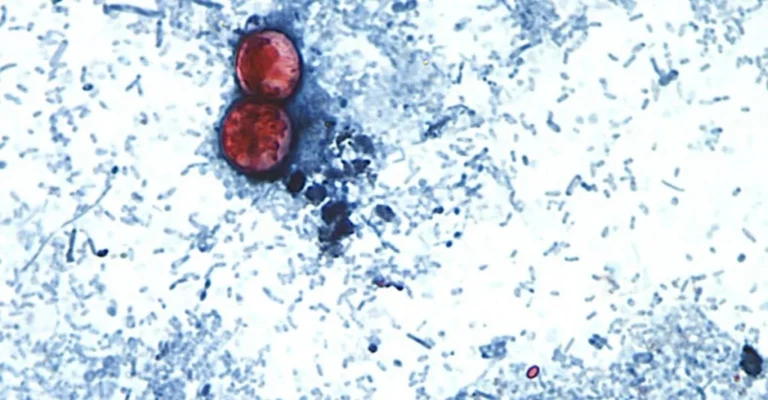
The current outbreak in eastern Congo and now Uganda is fueled by the Bundibugyo virus, a member of the Ebolavirus genus. Unlike more common strains that have been the subject of extensive international vaccine research, Bundibugyo presents a unique, terrifying challenge: it is historically elusive and lacks the medical countermeasures—such as the rVSV-ZEBOV vaccine—that have been deployed in previous outbreaks.
The virus is transmitted through direct contact with the bodily fluids of infected individuals—living or deceased. Healthcare workers and family caregivers remain the most vulnerable populations. Symptoms typically manifest as hemorrhagic fever, characterized by internal and external bleeding, organ failure, and a high mortality rate if left untreated in the early stages.
The Ugandan government’s decision to seal the border, while drastic, highlights the tension between public health directives and political reality. While the World Health Organization (WHO) warns that border closures often force populations to use informal, unmonitored footpaths—thereby increasing the risk of uncontrolled spread—Uganda’s task force has opted for a "hard" containment strategy to prevent the further influx of infected individuals.
Chronology of the Outbreak
The trajectory of this crisis has been marked by delays, misdiagnosis, and the compounding effects of regional instability.
- Mid-May: The outbreak begins in eastern Congo. Initial diagnostic efforts are hampered because testing protocols were calibrated for the more common Zaire strain of Ebola, leading to a critical delay in identifying the Bundibugyo variant.
- May 14: A 59-year-old man dies in Kampala, marking the first confirmed Ebola-related fatality in the Ugandan capital.
- May 15: The Democratic Republic of the Congo officially declares an Ebola outbreak in the eastern regions.
- Late May: Ugandan health authorities identify seven confirmed cases, several of which are linked to healthcare workers who treated Congolese patients who crossed the border prior to the official declaration.
- June (Present): Ugandan authorities issue a temporary, immediate border closure. Exceptions are granted only for medical evacuations, humanitarian aid, essential cargo, and security personnel. Any person entering under these emergency conditions is subject to a mandatory 21-day quarantine.
Supporting Data: By the Numbers
The scale of the crisis in the DRC is rapidly outpacing the response capacity of local and international health organizations.
- Confirmed Cases: According to the Congolese Ministry of Health, there are 101 laboratory-confirmed cases as of this week.
- Suspected Burden: The number of suspected cases in eastern Congo is nearing the 1,000 mark, with at least 220 suspected deaths reported.
- Contact Tracing: Health officials are currently monitoring over 3,000 individuals identified as high-risk contacts.
- Ugandan Infections: Uganda has reported seven confirmed cases, though the focus remains on the rising number of "secondary" exposures among family members of infected healthcare workers.
The statistics highlight a grim reality: the virus is moving faster than the responders can track, a sentiment echoed by the WHO, which describes the situation as a "public health emergency of international concern."
Official Responses and Strategic Friction
The Ugandan Stance
Dr. Diana Atwine has been the primary voice for the Ugandan government’s aggressive posture. Beyond the border closure, she has expressed frustration with public complacency. In a widely reported incident, she rebuked citizens who gathered in large, dense crowds to celebrate the success of European football teams, urging a return to strict hygiene protocols, such as the use of hand sanitizer and the abandonment of traditional handshaking.
The World Health Organization (WHO) Perspective
WHO Director-General Tedros Adhanom Ghebreyesus has taken a diplomatic but firm stance. While acknowledging the high risk of contagion, he has called for a ceasefire in eastern Congo. He argues that persistent conflict in the region—characterized by attacks on clinics and the harassment of health volunteers—makes the systematic tracking of contacts "nearly impossible."
The WHO maintains that formal border closures are counterproductive. Their data suggests that when official checkpoints close, the movement of people and goods simply shifts to the hundreds of miles of porous, unmonitored footpaths that crisscross the Uganda-Congo border, effectively rendering the closure a "leaky" barrier.
International Intervention
In a significant shift in logistics, the United States government announced it would cease flying American citizens exposed to the virus directly to the U.S. Instead, the Trump administration is preparing a specialized containment facility in Kenya to serve as a regional hub for medical evacuations. This pivot underscores the global concern regarding the potential for international transmission.
Implications: A Region in Crisis
The Failure of Infrastructure and Funding
The current outbreak is not occurring in a vacuum. It is the result of years of systemic underfunding and regional instability. Health experts point to significant aid cuts implemented last year by the U.S. and other wealthy nations as a major contributor to the current lack of protective gear, such as face shields, specialized body bags, and diagnostic testing kits.
Security and Social Trust
The humanitarian response is being actively sabotaged by a lack of trust. In many parts of eastern Congo, local residents, having survived years of civil war and exploitation, view international health responders with deep suspicion. This has led to the stoning of ambulances and the destruction of clinics. When health workers are perceived as "outsiders" rather than healers, the medical response inevitably fails.
The Economic Cost
For the border communities of Uganda and Congo, the economic impact is immediate. The border regions thrive on cross-border trade and the movement of families. A long-term closure threatens the livelihood of thousands who rely on daily interaction for survival. The longer the border remains shut, the greater the pressure on local economies and the higher the likelihood of social unrest.
Conclusion: A Precarious Future
The situation remains fluid. While the recovery of the first patient in the town of Rwampara offers a sliver of hope, the fundamental problems remain: the virus is circulating in a war-torn, under-resourced region where health responders are struggling to gain the trust of the population.
As Uganda maintains its tight grip on the border, the international community faces a difficult choice: continue to press for open borders to facilitate aid and monitoring, or support the isolationist tactics that prioritize domestic containment at the expense of regional cooperation. One thing is certain: until a ceasefire is reached and the medical supply chain is secured, the Bundibugyo strain of Ebola will continue to pose a formidable challenge to the stability of East Africa.