






By Helen Branswell
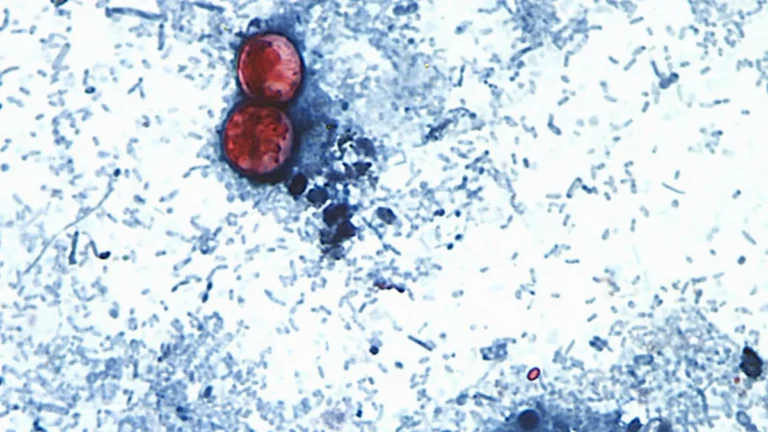
As a new, concerning outbreak of the Ebola virus emerges within the Democratic Republic of Congo (DRC), public health officials and researchers are grappling with a significant medical gap: there are currently no licensed vaccines available to provide protection against the specific strain currently circulating. The virus in question, the Bundibugyo ebolavirus, has historically been one of the least understood and least addressed members of the filovirus family.
While the medical community has made monumental strides in combatting the Zaire ebolavirus—the strain responsible for the devastating 2014–2016 West African epidemic—these advancements have left a dangerous vacuum regarding other variants. As the death toll in the DRC rises, the international community, led by the Coalition for Epidemic Preparedness Innovations (CEPI), has mobilized a $62 million funding package to accelerate the development of three distinct vaccine candidates. However, experts warn that despite this urgent infusion of capital, the path from the laboratory to clinical trials remains months away, leaving local populations vulnerable in the interim.
Main Facts: The Current Landscape of the Outbreak
The Bundibugyo ebolavirus is a rare, highly lethal pathogen. Unlike the Zaire strain, for which the Merck-manufactured vaccine Ervebo has proven to be a game-changer, Bundibugyo has historically been sidelined in global vaccine research portfolios.
The primary challenge facing health authorities is the specificity of existing immunizations. Ervebo, the gold standard in Ebola prevention, is highly effective but functionally limited; it does not offer cross-protection against the Bundibugyo strain. Consequently, the current outbreak in the DRC represents not just a humanitarian crisis, but a stark illustration of the "neglected disease" trap. Because the virus has historically caused few outbreaks, commercial interest in developing a vaccine has been minimal, leading to a dangerous lack of preparedness when the pathogen inevitably emerges.
The $62 million in funding provided by CEPI is designed to bridge this gap, supporting three separate entities in their efforts to manufacture, scale, and test candidate vaccines. The goal is to move beyond the experimental phase and reach a point where clinical trials can confirm safety and efficacy in human populations.
A Chronology of the Bundibugyo Virus
Understanding the urgency of the current situation requires looking back at the sporadic and elusive nature of the Bundibugyo strain.

- 2007: The Discovery. The Bundibugyo ebolavirus was first identified following an outbreak in the Bundibugyo District of Western Uganda. It was the first time this specific species of the virus was documented in humans. It caused significant alarm due to the high mortality rate, yet the outbreak was contained relatively quickly, which perhaps contributed to it falling off the global radar.
- 2012: The Second Appearance. Five years later, the virus re-emerged, again in the DRC and Uganda. This second outbreak reinforced the fact that the virus was not a "one-off" event but a persistent threat lurking in the animal reservoir.
- 2013–2025: The Research Lull. During the period between the 2012 outbreak and the present, the global scientific community focused heavily on the Zaire and Sudan strains of Ebola, as well as the related Marburg virus. While vaccines for Zaire were fast-tracked following the 2014–2016 catastrophe, Bundibugyo remained in the shadow, with funding diverted to more frequent epidemic threats.
- May 2026: The Current Crisis. The emergence of the virus in the DRC has sparked a race against time. Public health experts are now working to determine the extent of the outbreak and the specific transmission chains, while simultaneously attempting to compress a decade’s worth of vaccine development into a matter of months.
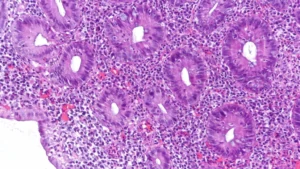
Supporting Data: Why Filoviruses are Formidable
The Ebolaviridae family is comprised of several distinct species, each with unique biological characteristics. The challenge in vaccine development lies in the fact that the immune response triggered by one species—such as the Zaire species—does not necessarily neutralize the Bundibugyo species.
Data from previous outbreaks suggest that the case fatality rate for Bundibugyo can range from 30% to 50%. While this is lower than the near-90% fatality rate sometimes seen with the Zaire strain, the lack of a specific vaccine or therapeutic means that supportive care—which is often limited in remote regions—remains the only line of defense.
The $62 million CEPI investment is being allocated toward:
- Platform Technology: Utilizing existing viral-vector platforms (similar to those used in COVID-19 and Zaire Ebola vaccines) to expedite the creation of a Bundibugyo-specific antigen.
- Manufacturing Scale-up: Investing in the supply chain to ensure that if a trial is successful, the vaccine can be produced in sufficient quantities for mass distribution.
- Clinical Trial Preparedness: Establishing the regulatory and logistical frameworks in the DRC so that the moment a candidate is ready for human testing, it can be deployed immediately.
Official Responses and Strategic Challenges
Public health organizations, including the World Health Organization (WHO) and CEPI, have been vocal about the systemic issues this outbreak highlights.
"We are essentially playing catch-up with a virus that has been known to us for nearly two decades," said one senior researcher involved in the CEPI-funded initiative. "The issue isn’t a lack of scientific capability; it is a lack of sustained, long-term investment in pathogens that don’t make headlines every year."
The WHO has emphasized that while the funding is a significant step forward, the "clinical trial" phase is the most arduous. Navigating the regulatory landscape in the DRC, ensuring ethical oversight in a conflict-prone or geographically isolated area, and maintaining a cold chain for vaccines in tropical climates are monumental logistical hurdles.
Furthermore, the scientific community is debating whether to pursue a "multivalent" vaccine—a single shot that protects against multiple species of Ebola—or to continue with species-specific development. While a multivalent vaccine would be the "holy grail" of filovirus research, it is technically more complex and further from reality than the current efforts to target Bundibugyo directly.
The Implications: Lessons for Future Preparedness
The current Bundibugyo outbreak serves as a sobering reminder of the flaws in our global health security infrastructure. We have moved toward a "reactive" model of epidemic response, where the world mobilizes only after a threat has materialized.
1. The Cost of Neglect
The financial burden of responding to an active outbreak is exponentially higher than the cost of funding proactive research. The $62 million being spent now is an emergency measure; had a fraction of that been invested in Bundibugyo vaccine research over the last decade, we might already have a licensed product ready for deployment.
2. Strengthening Health Systems
Vaccines are not a silver bullet. The success of any vaccination campaign in the DRC will depend entirely on the strength of the local healthcare infrastructure. This includes the ability to conduct contact tracing, provide supportive care to the sick, and gain the trust of local communities who may be wary of foreign medical interventions.
3. Global Equity
There is an ethical dimension to this struggle. The Bundibugyo virus disproportionately affects some of the world’s most vulnerable populations. The international community has a moral obligation to ensure that the fruits of modern biotechnology—specifically the rapid development of vaccines—are not reserved for the wealthy or for the most "globally significant" pathogens.
4. Future-Proofing
As climate change alters animal habitats and human encroachment into forests increases, the risk of zoonotic spillover (diseases jumping from animals to humans) is rising. We are likely to see more outbreaks of "rare" viruses. A move toward universal vaccine platforms—technologies that can be quickly adapted to new pathogens—is the only way to avoid being perpetually caught off guard.
Conclusion
As the DRC battles the current Bundibugyo outbreak, the world watches with a mix of anxiety and hope. The $62 million in funding is a vital, albeit belated, acknowledgement that every life in the path of this virus matters. While the clinical trials are months away, the work happening in laboratories today represents the best chance to prevent the next great epidemic.
The lesson is clear: in the world of infectious disease, "rare" is not synonymous with "safe." True global preparedness requires that we look beyond the headlines and invest in the science of the forgotten, ensuring that when the next outbreak inevitably arrives, we are ready to meet it with more than just good intentions. The race to vaccinate against the Bundibugyo virus is not just a scientific endeavor; it is a test of our collective resolve to leave no one behind in the face of a viral threat.