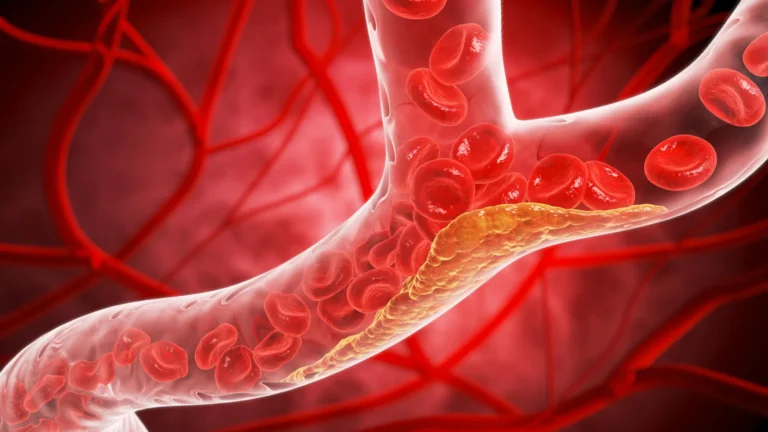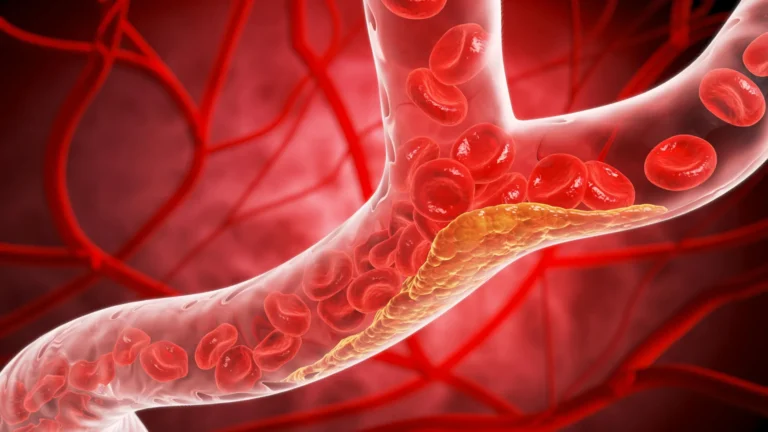








In a significant challenge to current cardiovascular clinical practice, a new study led by researchers at the Icahn School of Medicine at Mount Sinai has unveiled a concerning diagnostic gap: the most widely used tools for assessing heart attack risk fail to identify nearly half of the patients who go on to suffer a cardiac event. The findings, published on November 21 in the Journal of the American College of Cardiology: Advances, suggest that current medical guidelines—which rely heavily on population-based risk calculators and symptom reporting—may be fundamentally ill-equipped to safeguard individual patients.
The study, which scrutinized the real-world performance of established risk assessment models, indicates that millions of individuals may be receiving a false sense of security during routine physicals. By the time a patient experiences the classic warning signs of a heart attack, the window for effective, non-invasive intervention has often already closed.
The Pillars of Modern Screening: A Critical Evaluation
For decades, primary care physicians have relied on two primary metrics to determine a patient’s heart health: the Atherosclerotic Cardiovascular Disease (ASCVD) risk score and, more recently, the PREVENT equations. These tools are designed to categorize patients based on statistical probabilities, factoring in variables such as age, sex, ethnicity, blood pressure, cholesterol levels, diabetes status, and smoking history.
The ASCVD score is the standard-bearer for estimating the likelihood of a major adverse cardiovascular event over a 10-year period. Physicians use these scores to decide if a patient should be prescribed preventive measures, such as statins or aggressive blood pressure management. When a patient falls into the "low" or "borderline" risk category—and lacks overt symptoms like chest pain or shortness of breath—they are typically discharged with a clean bill of health.
However, the Mount Sinai research team sought to stress-test these tools against actual clinical outcomes. By evaluating 474 patients under the age of 66 who had no prior history of coronary artery disease but were admitted for their first heart attack, the researchers were able to "reverse engineer" the patients’ risk profiles. They simulated how these individuals would have been assessed by their physicians just 48 hours before their cardiac emergencies. The results were stark: standard guidelines would have left a massive portion of these patients without treatment or further investigation.
Chronology of a Crisis: The 48-Hour Gap
The study’s methodology provides a chilling look at the timeline of heart disease. By analyzing 474 patients treated at Mount Sinai Morningside and The Mount Sinai Hospital between January 2020 and July 2025, the researchers created a timeline of clinical interactions versus physiological reality.
- The Baseline (Pre-Event): The researchers collected comprehensive demographic, biometric, and clinical data for each subject.
- The Simulated Consultation: They applied the ASCVD and PREVENT calculators to each patient’s data as if they were standing in a clinic two days before their heart attack.
- The Clinical Reality: Using medical records, the team tracked the exact onset of symptoms for each patient.
- The Findings: 45% of patients would not have qualified for preventive therapy under ASCVD guidelines. That number jumped to 61% under the newer PREVENT tool. Furthermore, 60% of these patients reported no symptoms until fewer than two days before their heart attack.
This chronology exposes a "prevention paradox." Because these tools are designed to filter patients based on population-wide averages, they are inherently prone to missing the "outlier"—the individual who may have sub-clinical, silent atherosclerosis that is nonetheless primed for rupture.
Supporting Data: Why Risk Calculators Fall Short
The data highlights a significant discrepancy between "population health" and "individual medicine." While ASCVD and PREVENT are excellent at identifying broad groups of people who might be at risk, they fail to account for the physical presence of plaque within the arterial walls.
"Our research shows that population-based risk tools often fail to reflect the true risk for many individual patients," explains Dr. Amir Ahmadi, the study’s corresponding author and a Clinical Associate Professor of Medicine (Cardiology) at the Icahn School of Medicine at Mount Sinai.
The study categorized patients into four risk tiers: low (<5%), borderline (5–7.5%), intermediate (7.5–20%), and high (>20%). The data revealed that the majority of the patients who suffered a first heart attack were actually categorized as low or intermediate risk by these calculators.
If a patient is categorized as "low risk," they are rarely offered advanced diagnostic testing. The study suggests that because 60% of the patients only developed symptoms within 48 hours of their event, the current system is essentially waiting for the disease to reach an advanced, symptomatic stage before it triggers a clinical response. By then, the "prevention" phase is over, and the "emergency treatment" phase has begun.
Official Perspectives: Shifting the Paradigm
The investigators are calling for a fundamental shift in how medicine views "prevention." Rather than waiting for a risk score to reach a specific threshold or for a patient to complain of chest pressure, the authors argue that the focus must shift to early, direct detection of the underlying disease.
"This study suggests that the current approach of relying on risk scores and symptoms as primary gatekeepers for prevention is not optimal," Dr. Ahmadi asserts. "It may be time to fundamentally reconsider this model and move toward atherosclerosis imaging to identify the silent plaque—early atherosclerosis—before it has a chance to rupture."
Dr. Anna Mueller, the study’s first author and an internal medicine resident at Mount Sinai, emphasizes the danger of relying on symptomatic presentation. "When we look at heart attacks and trace them backwards, most heart attacks occur in patients in the low or intermediate risk groups," she notes. "This study highlights that a lower risk score, along with not having classic heart attack symptoms, is no guarantee of safety on an individual level."
For the medical community, this represents a call to action. The current guidelines are not necessarily "wrong" for identifying large swaths of high-risk individuals, but they are insufficient for the purpose of absolute prevention in the individual patient.
Implications for Future Cardiovascular Care
The implications of this research are far-reaching, potentially influencing everything from insurance coverage to standard clinical guidelines.
1. The Role of Imaging
The study strongly suggests that cardiovascular imaging (such as coronary artery calcium scoring or CT angiography) should play a more central role in risk assessment. Unlike risk calculators, which only estimate the probability of disease, imaging provides a direct view of the presence of disease. Identifying plaque early allows for immediate, aggressive lifestyle and pharmacological interventions that could potentially halt or reverse the progression of atherosclerosis.
2. Redefining "Symptomless"
Medicine has long treated the absence of symptoms as evidence of health. The Mount Sinai study proves this is a dangerous fallacy. If 60% of heart attack victims are asymptomatic until the final 48 hours, then the absence of symptoms must be reclassified as a period of "silent progression" rather than a period of safety.
3. Personalized Medicine
The researchers acknowledge that more work is required to refine these diagnostic strategies. Large-scale, prospective studies are needed to determine how to integrate imaging into routine primary care without overwhelming the healthcare system with unnecessary testing. The goal is to create a more nuanced "risk profile" that balances the accuracy of imaging with the efficiency of current calculators.
4. A Wake-up Call for Patients
For the general public, the study serves as a reminder that a "low" score on a routine physical does not grant immunity from heart disease. Individuals, particularly those with a family history or other risk factors, should advocate for a more proactive discussion with their physicians about their cardiovascular health, potentially inquiring about advanced screening methods beyond the standard blood pressure and cholesterol panels.
Conclusion
The findings from Mount Sinai represent a critical inflection point in cardiology. By exposing the limitations of standard risk assessment tools, the researchers have provided a compelling case for a more personalized, imaging-based approach to cardiac care.
While risk calculators will likely remain a part of the clinician’s toolkit, they can no longer be the sole gatekeepers of preventive medicine. As medical technology continues to evolve, the ability to "see" the disease before it manifests as a clinical event offers the best hope for reducing the global burden of heart attacks. The future of heart health, it seems, lies not in calculating the odds of a heart attack, but in identifying and neutralizing the silent threat of atherosclerosis before it ever has the chance to strike.