In the life-or-death landscape of organ transplantation, the system designed to distribute donor lungs is intended to be a beacon of equity, prioritizing the sickest patients and ensuring the highest biological compatibility. However, a landmark study conducted by researchers at the Cleveland Clinic and Case Western Reserve University, recently published in the journal CHEST, has cast a shadow on the effectiveness of recent reforms to the national lung allocation system.
The research indicates that despite systemic updates intended to streamline the process, geographic location remains a primary determinant of a patient’s survival prospects. The findings suggest that current policy amendments—specifically those that prioritize geographic proximity—may be inadvertently widening the gap between patients in different regions, potentially penalizing those living in areas with lower donor density.
The Core Problem: A Postcode Lottery for Organs
The fundamental challenge in lung transplantation is the inherent scarcity of donor organs. Every day, individuals with end-stage lung disease are added to a waitlist that consistently outpaces the supply of viable lungs. To manage this crisis, the United States utilizes the Composite Allocation Score (CAS). This metric acts as a weighted algorithm, evaluating candidates based on three critical pillars: medical urgency, projected post-transplant survival, and biological compatibility.
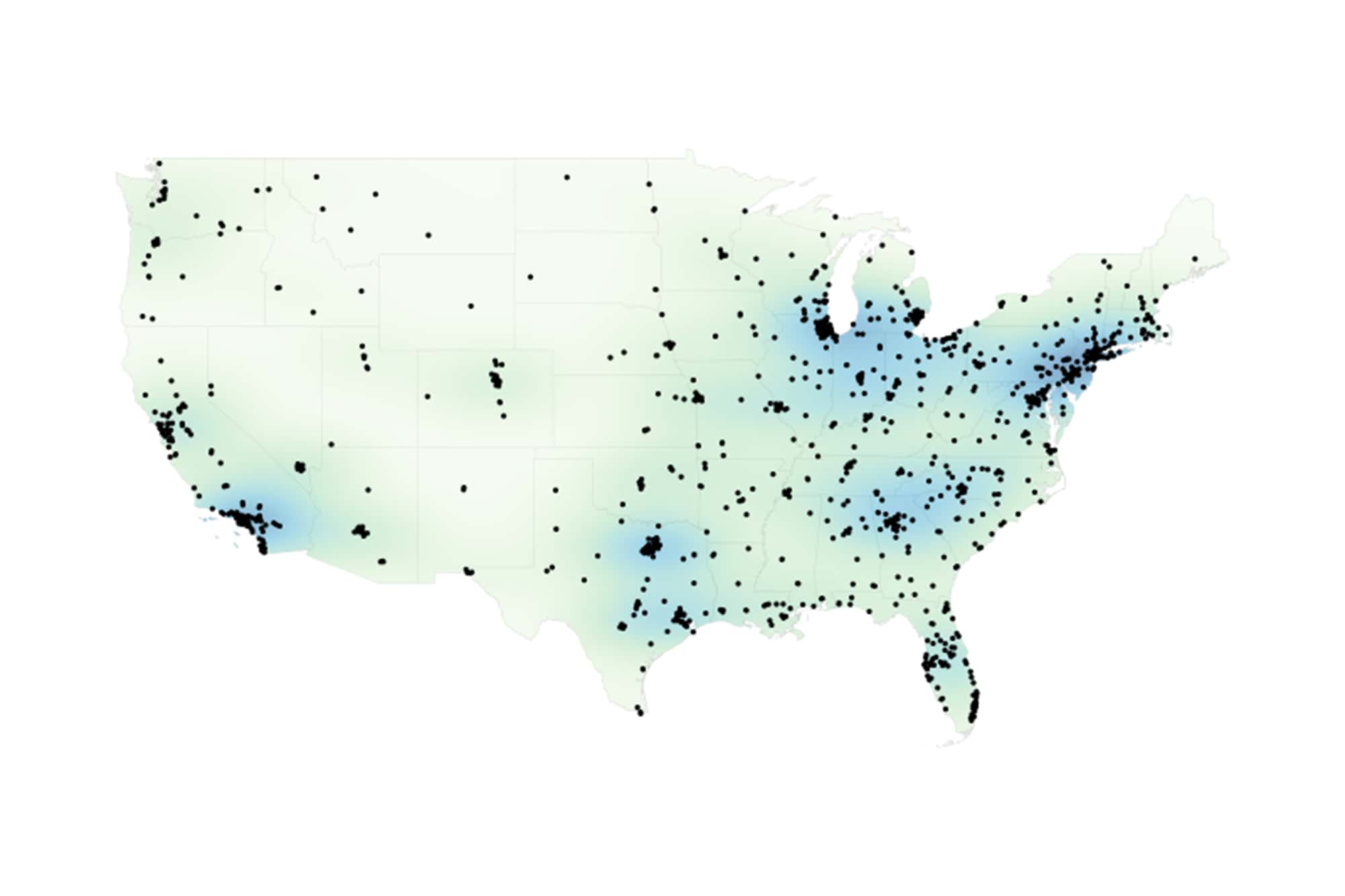
For years, the medical community has sought to refine the CAS to make it more equitable. However, the study from the Cleveland Clinic highlights a persistent, uncomfortable truth: the "geography of hope" remains uneven. When researchers analyzed 3,917 adult lung transplant candidates across 61 U.S. transplant centers, they discovered that an individual’s ability to receive a life-saving transplant is still heavily dictated by their location on the map.
Chronology of a Shifting Policy Landscape
To understand the implications of the new study, one must look at how the allocation system has evolved over the last decade.
- Pre-2020 Era: Historically, organ allocation relied heavily on localized "donor service areas" (DSAs). This created significant disparities where organs might be offered to patients within a specific region before being offered to a sicker patient just across a state line.
- The Transition to CAS: The implementation of the Composite Allocation Score was designed to move away from rigid geographic boundaries, aiming for a more nationalized, needs-based approach.
- The Proximity Shift: Most recently, regulatory bodies introduced amendments to the CAS that place a higher priority on "geographic efficiency"—specifically, the proximity between the donor hospital and the candidate. The rationale was to minimize cold ischemic time (the time an organ spends outside the body), which is crucial for transplant success.
- The 2026 Findings: The current research serves as an empirical audit of these recent amendments. By modeling the effects of prioritizing distance, researchers found that this "efficiency" may come at a high cost to equity, effectively re-introducing the geographic barriers the system originally set out to dismantle.
Supporting Data: The Disparity in Numbers
The research team employed a novel metric dubbed "distance-adjusted donor availability." This allowed them to quantify the pool of compatible donors for any given center, adjusted for the proximity-based weighting of the current policy.
Regional Variance
The data reveals a stark divide. Centers located in the Western United States were found to have 30% lower "effective donor availability" compared to their counterparts in the Midwest. This suggests that a patient listed at a hospital in the West faces a significantly steeper climb to receive a lung offer than a patient with similar medical urgency in the Midwest or parts of the South.
The "Match-Run" Disruption
Perhaps the most concerning discovery in the CHEST study involves the "match-run" analysis. When researchers simulated how the amended proximity-based policy changes the ranking of candidates, they found that 23.9% of patients who were previously in the "top 10" for an organ offer were displaced from those top positions.
This is not merely a statistical shift; it is a clinical one. It suggests that, under the new rules, the most critically ill patients—who would have otherwise been at the front of the line—are being passed over in favor of patients who happen to be geographically closer to the donor, regardless of the relative urgency of their conditions.
The Vulnerability of Specific Demographics
The study further identified that certain groups are disproportionately impacted by the shift toward proximity. Patients with "difficult-to-match" biological profiles, such as those with blood type O, face the greatest levels of de-prioritization. Because these patients already have a smaller pool of compatible donors, adding a geographic filter creates a double-jeopardy scenario that further restricts their access to life-saving organs.
Official Responses and Clinical Perspectives
The medical community has reacted to these findings with a mix of urgency and calls for nuanced reform.
Dr. Maryam Valapour, director of lung transplant outcomes at Cleveland Clinic and a lead author of the study, emphasized the complexity of the dilemma. "Our analysis found that access to donor lungs continues to vary across the country," Dr. Valapour stated in a press release. She highlighted that while the goal of increasing efficiency is noble, the unintended consequences cannot be ignored. "Placing greater emphasis on how close a patient is to a donor hospital may make it harder for some patients to receive compatible donor lungs. This is important because while lung transplants have been increasing, there is still a shortage of organs, and more people are added to the wait list every day."
Dr. Jarrod Dalton, director of the Center for Populations Healthcare Research at Cleveland Clinic, echoed these sentiments, pointing to the systemic nature of the issue. "Although the national lung allocation system has evolved in recent years, our findings suggest meaningful regional differences in donor access remain," Dr. Dalton noted. He underscored that the changes favoring proximity may be doing more harm than good for those who have the fewest options to begin with.
Implications: The Future of Transplant Policy
The findings of this study present a significant challenge to policymakers at the Organ Procurement and Transplantation Network (OPTN) and other oversight bodies.
The Efficiency vs. Equity Trade-off
The core of the debate is a classic ethical trade-off: clinical efficiency versus distributive justice. Proximity-based allocation is undeniably efficient; it reduces the risk of graft injury by shortening transit times. However, the study makes a compelling case that this efficiency is being purchased at the cost of equity. If a patient is dying of respiratory failure, the priority should arguably be their physiological need, not their travel distance from the donor site.
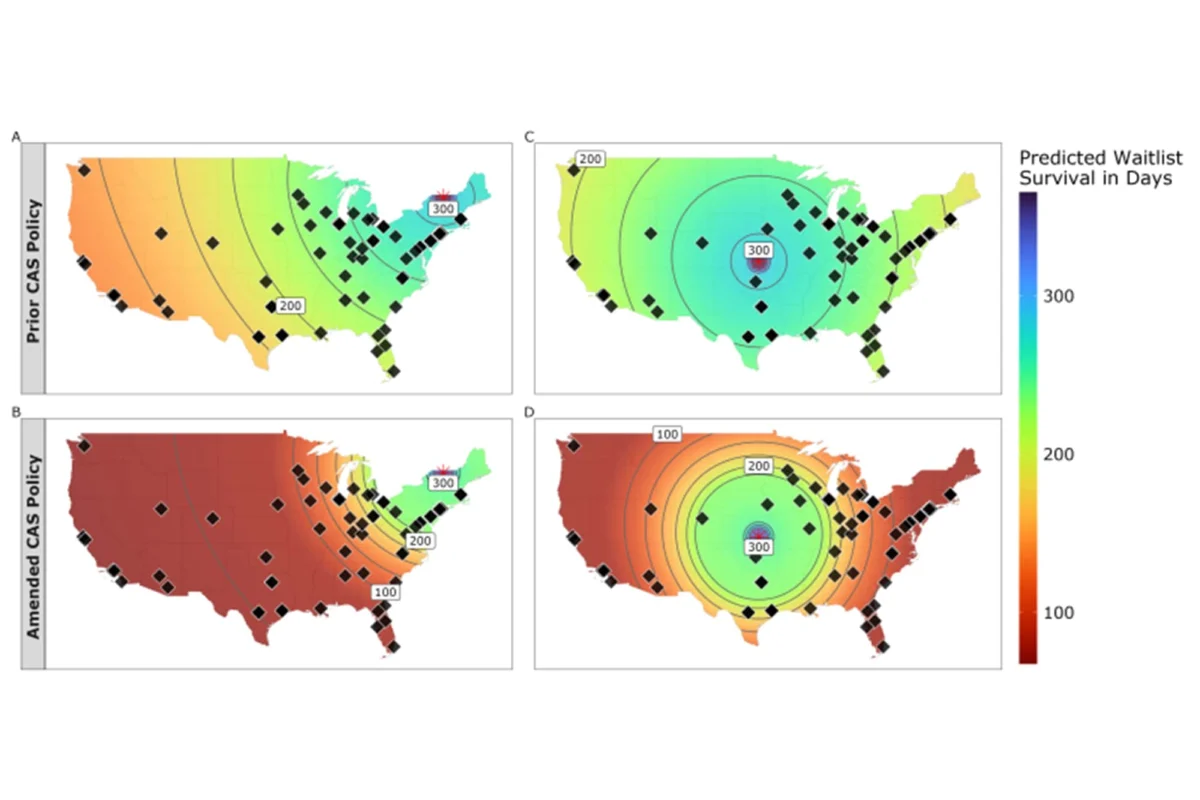
Re-evaluating the "Distance-Urgency" Trade-off
The study’s visual models demonstrate that the current policy creates a rigid trade-off between how sick a patient is and how far they are from a donor. The researchers argue that by tightening the "distance" variable, the system is essentially forcing surgeons and coordinators to overlook the most urgent cases in favor of logistical convenience.
Policy Recommendations
While the study does not explicitly call for the repeal of the proximity rule, it strongly suggests that the weight given to distance must be reconsidered. Experts are now calling for:
- Increased Transparency: A more public accounting of how proximity weighting impacts waitlist mortality in specific regions.
- Adaptive Algorithms: Developing "smarter" allocation models that prioritize proximity only when the clinical benefit of reduced ischemic time outweighs the urgency of the patient’s condition.
- Regional Support: Targeted interventions to bolster donor recovery rates in regions like the West, which currently lag behind the rest of the country in effective donor availability.
Conclusion: A Call for Refined Equity
The Cleveland Clinic/Case Western Reserve study is a sobering reminder that policy in the medical field often has unintended consequences. While the national lung allocation system has certainly made progress in professionalizing and standardizing the way organs are matched, the goal of a truly "fair" system remains elusive.
As the medical community digests these findings, the conversation must shift toward a more sophisticated model of allocation—one that recognizes the importance of geographic efficiency but refuses to sacrifice the lives of the most vulnerable patients on the altar of logistics. The search for a balanced system is not just an academic exercise; for the thousands of patients waiting for the gift of breath, it is the defining factor of their survival. The path forward requires a delicate recalibration, ensuring that where a patient lives does not dictate whether they live.