






In the landscape of modern medicine, chronic pain and hypertension have long been viewed as distinct clinical entities—one a sensory experience often managed by pain specialists, the other a cardiovascular condition governed by cardiologists. However, groundbreaking research published in the American Heart Association’s journal Hypertension suggests that these two conditions are far more intertwined than previously understood.
A comprehensive study of over 200,000 U.S. adults has unveiled a critical correlation: chronic pain, particularly when widespread, acts as a significant risk factor for the development of high blood pressure. By analyzing the intersection of physical discomfort, psychological health, and systemic inflammation, researchers have opened a new door for preventative cardiology.
The Core Findings: A Quantitative Look at Pain and Pressure
The research, led by Dr. Jill Pell, the Henry Mechan Professor of Public Health at the University of Glasgow, provides a longitudinal perspective on how pain manifests as a cardiovascular threat. Over an average follow-up period of 13.5 years, the study tracked participants who reported chronic pain—defined as discomfort lasting at least three months that interfered with daily life.
The findings were unequivocal: the "dosage" of pain matters. Individuals experiencing chronic pain throughout their entire bodies demonstrated a statistically significant increase in the likelihood of developing high blood pressure compared to those with localized pain, short-term discomfort, or no pain at all.
"The more widespread their pain, the higher their risk of developing high blood pressure," Dr. Pell stated. This discovery shifts the narrative from viewing pain as a localized symptom to understanding it as a systemic physiological stressor.
The Psychological Pathway: The Depression-Hypertension Axis
Perhaps the most revealing aspect of the study is the identification of depression as a "mediator" in the relationship between pain and blood pressure. The research team found that chronic pain frequently serves as a gateway to depression, which in turn elevates cardiovascular risk.
"Part of the explanation for this finding was that having chronic pain made people more likely to have depression, and then having depression made people more likely to develop high blood pressure," Dr. Pell explained.
This tripartite relationship—Pain → Depression → Hypertension—suggests that the mental health implications of chronic physical suffering are not merely secondary concerns; they are fundamental drivers of heart health. Consequently, the study advocates for a more integrated clinical approach. If physicians can identify and treat depressive symptoms early in patients presenting with chronic pain, they may simultaneously be lowering those patients’ risk of developing stage one or stage two hypertension.
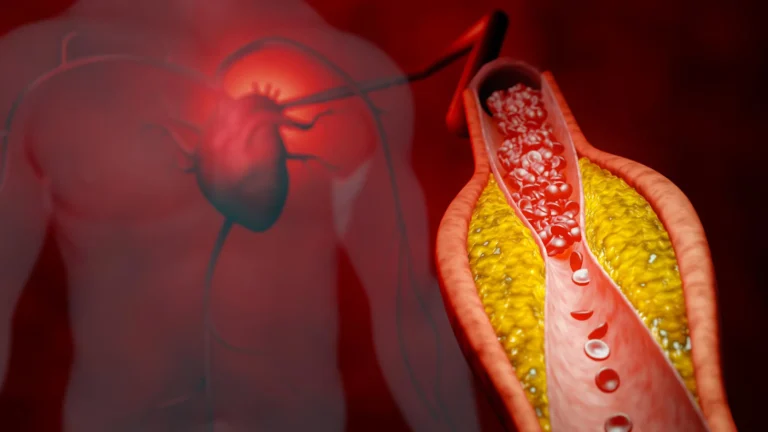
The Cardiovascular Stakes: Understanding the Threat
To understand the gravity of these findings, one must look at the lethality of hypertension itself. According to the 2025 joint guidelines from the American Heart Association and the American College of Cardiology, high blood pressure is the leading cause of death both nationally and globally.
Hypertension, categorized by readings of 130/80 mm Hg or higher, places excessive mechanical stress on the walls of blood vessels. Over time, this constant force leads to vascular damage, increasing the risk of myocardial infarction (heart attack), stroke, and kidney failure. With nearly half of all U.S. adults currently living with some form of hypertension, the revelation that chronic pain is a contributing factor adds a massive new cohort to the "at-risk" population.
Methodology: Tracking the Long-Term Impact
The study’s robust design allowed for a deep dive into the demographics of pain. Participants were asked at baseline to identify the specific locations of their pain—including the head, face, neck/shoulder, back, stomach/abdomen, hip, and knee. Researchers then correlated this data with clinical diagnostic coding over a 13.5-year period.
Assessing the Biological Markers
The research team went beyond self-reporting by utilizing objective clinical measures:
- Depression Screening: Participants were evaluated for mood, disinterest, restlessness, and lethargy.
- Inflammation Testing: Researchers measured C-reactive protein (CRP) levels, a primary biomarker for systemic inflammation.
- Blood Pressure Monitoring: Clinical measurements were taken at follow-up intervals to track the emergence of hypertension.
By integrating these metrics, the study confirmed that inflammation—a known accomplice in the development of hypertension—is heavily influenced by the presence of long-term pain.
Expert Perspectives: A Paradigm Shift in Pain Management
Dr. Daniel W. Jones, chair of the 2025 AHA/ACC High Blood Pressure Guideline, emphasized that while the short-term spikes in blood pressure caused by acute pain are well-documented, the long-term impact of chronic pain has remained a "missing link" in cardiovascular health.
"This study adds to that understanding, finding a correlation between the number of chronic pain sites and that the association may be mediated by inflammation and depression," Dr. Jones noted.
However, Dr. Jones also raised a critical concern regarding how we treat the pain itself. He highlighted the potential for "iatrogenic harm"—damage caused by the treatment. "Chronic pain needs to be managed within the context of the patients’ blood pressure, especially in consideration of the use of pain medication that may adversely affect blood pressure," he warned.
Specifically, nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, which are the standard of care for many forms of musculoskeletal pain, are known to increase blood pressure. This creates a clinical "catch-22": the medication used to treat the pain may inadvertently accelerate the very condition the physician is trying to prevent.
Implications for Clinical Practice
The message for healthcare providers is clear: treat the patient, not just the symptom. The study suggests that the current siloed approach to medicine—where a pain specialist treats the back and a cardiologist treats the heart—is insufficient.
Recommendations for Providers:
- Screen for Comorbidities: Patients presenting with musculoskeletal pain should be screened for symptoms of depression and monitored for rising blood pressure.
- Pharmacological Vigilance: Physicians must exercise caution when prescribing NSAIDs to patients who are already at risk for or diagnosed with hypertension.
- Holistic Management: Pain management strategies should prioritize non-pharmacological interventions, such as physical therapy, cognitive-behavioral therapy (CBT), and exercise, which may address the pain without the cardiovascular side effects of long-term medication use.
Study Limitations and Future Directions
Despite the study’s significant impact, the authors acknowledged several limitations that warrant future investigation. The participant pool consisted primarily of middle-aged and older white adults of British origin. This homogeneity suggests that the findings may not be fully representative of younger populations or diverse racial and ethnic groups, who may experience pain and hypertension through different sociocultural and biological lenses.
Furthermore, the study relied on self-reported pain levels and a single baseline assessment. Future research, as recommended by Dr. Jones, should employ randomized controlled trials to determine the direct causal relationship between specific pain management strategies and long-term blood pressure outcomes.
Conclusion: A New Frontier in Preventive Medicine
The research published in Hypertension serves as a wake-up call for both patients and providers. Chronic pain is not merely a signal of physical damage; it is a systemic warning sign that the body is under long-term stress.
As we move forward, the integration of mental health support, careful pharmacological management, and proactive cardiovascular screening for chronic pain sufferers will be essential. By treating the whole patient—addressing the inflammatory and psychological roots of pain—the medical community can potentially mitigate one of the most pervasive, yet preventable, drivers of global mortality.
In the words of Dr. Pell: "When providing care for people with pain, health care workers need to be aware that they are at higher risk of developing high blood pressure, either directly or via depression. Recognizing pain could help detect and treat these additional conditions early."
The future of heart health, it seems, starts with listening to the pain.