In the landscape of modern preventive medicine, the "risk score" has long been considered the gold standard for cardiac health. By inputting variables like blood pressure, cholesterol, and age into standardized calculators, clinicians have for decades determined who requires life-saving statins or further diagnostic testing. However, a landmark study led by researchers at the Icahn School of Medicine at Mount Sinai has cast a shadow over this diagnostic framework, revealing that current screening methods may be failing a significant portion of the population.
The findings, published on November 21 in the Journal of the American College of Cardiology: Advances, suggest that nearly half of all individuals who suffer a heart attack would have been classified as "low" or "borderline" risk—and thus deemed ineligible for preventive intervention—just 48 hours before their cardiac event. This revelation strikes at the heart of current clinical guidelines, prompting a rigorous debate over whether it is time to abandon symptom-based assessment in favor of direct, imaging-based detection of silent arterial disease.
The Limitations of Conventional Wisdom
For years, the medical community has relied heavily on the atherosclerotic cardiovascular disease (ASCVD) risk score. This tool is designed to estimate the probability of a heart attack or stroke occurring within a 10-year window, factoring in demographic and biological data such as age, sex, race, blood pressure, cholesterol levels, diabetes status, and smoking history. More recently, a newer tool known as PREVENT has been introduced, aiming to provide a more nuanced picture by incorporating a broader array of variables.
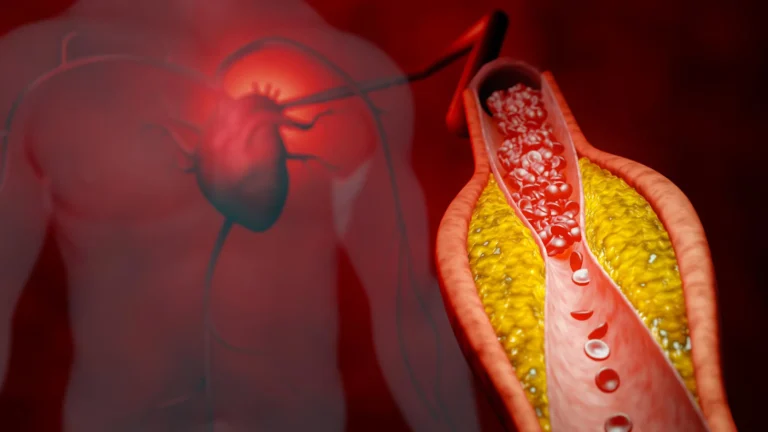
While these tools are exceptionally effective at identifying risk across large populations, the Mount Sinai study highlights a dangerous disconnect: what works for a population does not necessarily work for an individual. According to the research, relying on these statistical models as the primary "gatekeepers" for preventative care is failing to capture the reality of the individual patient, particularly those harboring "silent" atherosclerosis—plaque buildup that remains asymptomatic until the moment of a catastrophic event.
Chronology of the Investigation
The study was born from an urgent clinical observation: patients were arriving at Mount Sinai hospitals experiencing their first heart attack despite having had no prior history of coronary artery disease and, in many cases, no warning symptoms.
The Methodology
To investigate the gap between clinical scores and real-world outcomes, the research team conducted a retrospective analysis of 474 patients. These patients were all under the age of 66 and were treated for their first heart attack at either The Mount Sinai Hospital or Mount Sinai Morningside between January 2020 and July 2025.
The researchers performed a granular "time-travel" simulation for each patient. By utilizing the demographic and health data available to these patients just two days before their heart attacks, the team calculated what their ASCVD and PREVENT risk scores would have been at that precise moment. The patients were then sorted into four standard risk categories:
- Low: Under 5% 10-year risk
- Borderline: 5% to 7.5% 10-year risk
- Intermediate: 7.5% to 20% 10-year risk
- High: Over 20% 10-year risk
The goal was to determine if these patients would have triggered a clinical recommendation for preventive therapy, such as statins, or further diagnostic screening based on current medical guidelines.
Supporting Data: A Statistical Wake-Up Call
The results of the analysis were, by the authors’ own admission, sobering. The study revealed that when using the standard ASCVD risk score, 45% of the patients who suffered a heart attack would not have been recommended for any preventive therapy or further diagnostic testing.
The findings were even more pronounced when the newer PREVENT tool was applied. Under the PREVENT model, 61% of the patients would have fallen into the low or borderline risk categories.
Furthermore, the data regarding symptom onset provided a grim reality check for clinicians. The majority of patients (60%) reported that their symptoms began fewer than two days before the heart attack. This indicates that relying on symptoms like chest pain or shortness of breath as a primary indicator for medical intervention is fundamentally flawed. By the time these symptoms appear, the underlying atherosclerosis is typically already in an advanced, unstable state.
Official Responses and Clinical Perspectives
The lead researchers at Mount Sinai have been vocal about the implications of these findings, characterizing them as a call for a paradigm shift in cardiology.
The Case for Reconsideration
"Our research shows that population-based risk tools often fail to reflect the true risk for many individual patients," says Amir Ahmadi, MD, Clinical Associate Professor of Medicine (Cardiology) at the Icahn School of Medicine at Mount Sinai and the study’s corresponding author. "If we had seen these patients just two days before their heart attack, nearly half would NOT have been recommended for further testing or preventive therapy guided by current risk estimate scores and guidelines."
Dr. Ahmadi emphasizes that the "gatekeeper" model of cardiology—where a patient must meet a certain risk threshold to warrant advanced investigation—is no longer optimal. "It may be time to fundamentally reconsider this model and move toward atherosclerosis imaging to identify the silent plaque—early atherosclerosis—before it has a chance to rupture," he argues.
The Individual vs. The Population
First author Anna Mueller, MD, an internal medicine resident at the Icahn School of Medicine at Mount Sinai, notes that the discrepancy between low-risk classification and actual cardiac events is a major flaw in the current system.
"When we look at heart attacks and trace them backwards, most heart attacks occur in patients in the low or intermediate risk groups," Dr. Mueller explains. "This study highlights that a lower risk score, along with not having classic heart attack symptoms—which is common—is no guarantee of safety on an individual level. Our study exposes a major flaw where tools effective for tracking large populations fall short when guiding individualized care."
Implications: Moving Toward Early Detection
The implications of the Mount Sinai study are far-reaching, suggesting that the medical community must pivot from risk-based assessment to direct, structural assessment of the arteries.
From Risk Scores to Imaging
If risk calculators are insufficient, what is the alternative? The authors point toward cardiovascular imaging as the most promising frontier. Technologies such as coronary artery calcium (CAC) scoring and coronary CT angiography allow physicians to visualize the actual presence of plaque in the arteries. Unlike a risk score, which predicts the probability of a future event based on averages, imaging identifies the actual presence of disease.
The study advocates for a shift in focus: doctors should move away from detecting "symptomatic" heart disease and toward detecting the "silent" disease that is currently invisible to our standard screening tools.
Future Directions and Research
The researchers acknowledge that this study is not the final word on the matter. While the data provides a strong argument for change, further work is required to refine these methods and determine the best way to integrate imaging into routine primary care.
Future research will likely focus on:
- Cost-Effectiveness: Analyzing the economic impact of widespread imaging versus the high cost of treating heart attacks and their long-term complications.
- Protocol Development: Determining at what age or risk profile imaging should be mandated to maximize the detection of silent plaque.
- Refining Risk Tools: Investigating if existing risk scores can be combined with imaging data to create a more accurate, hybrid diagnostic model.
Conclusion
The Mount Sinai study serves as a critical reminder that medical guidelines, while essential for managing public health, are not absolute indicators of individual safety. As medicine moves toward a more personalized, precision-based approach, the reliance on statistical averages may be giving patients a false sense of security.
By identifying that a large majority of first-time heart attack victims are being "missed" by current guidelines, the researchers have provided a compelling mandate: it is time to look closer. Moving toward a model that prioritizes the early detection of plaque—rather than waiting for a patient to reach a certain threshold of risk or symptoms—could represent the next great leap in reducing the global burden of cardiovascular disease. The message is clear: the absence of a high-risk score is not the same as the absence of disease, and for many patients, the time to act is long before the first symptom appears.