








For the first time since 2018, the medical community has received a comprehensive update to the clinical gold standard for managing cardiovascular health. The American College of Cardiology (ACC) and the American Heart Association (AHA) have released new, rigorous guidance on the screening and management of blood cholesterol. Unveiled on March 28 at the ACC’s 75th Annual Scientific Session in New Orleans and published simultaneously in the Journal of the American College of Cardiology and Circulation, these recommendations represent a fundamental shift in how clinicians approach the primary and secondary prevention of heart disease.
This update, complemented by a seminal paper titled "The ABCs of Cardiovascular Disease Prevention: Communicating What We Know in 2026" in the American Journal of Preventive Cardiology, arrives at a critical juncture. With cardiovascular disease remaining the leading cause of mortality globally, the new guidelines prioritize aggressive, personalized, and earlier intervention to combat the silent progression of atherosclerosis.
The Core Mandate: Why 2026 Demands a New Approach
The fundamental objective of the 2026 guidelines is clear: lower low-density lipoprotein (LDL) cholesterol—the "bad" cholesterol—with greater precision and urgency. However, the guidelines go beyond simple LDL metrics. They now place a renewed focus on other atherogenic blood fats, most notably lipoprotein(a) or Lp(a), and emphasize that cardiovascular health must be viewed through the lens of a patient’s entire life course rather than a snapshot taken in middle age.
"We know that lower LDL cholesterol levels are better when it comes to reducing the risk of heart attacks, strokes and congestive heart failure," explains Dr. Roger S. Blumenthal, chair of the guideline writing committee and director of the Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease. "We also know that bringing elevated lipids and blood pressure down in young adults supports optimal heart and vascular health throughout a person’s life."
The Burden of Disease
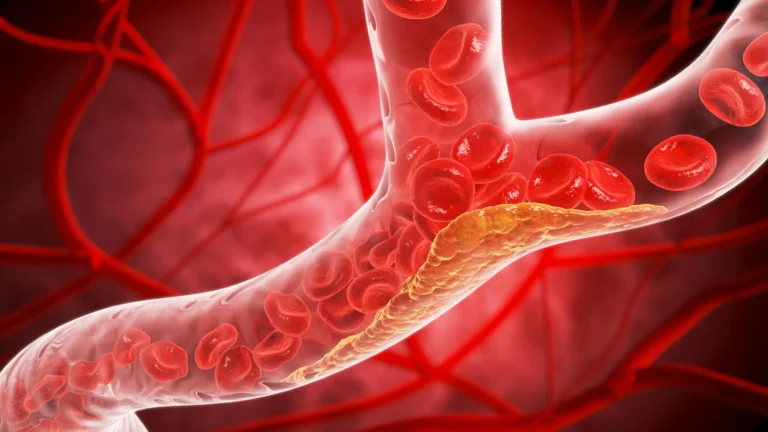
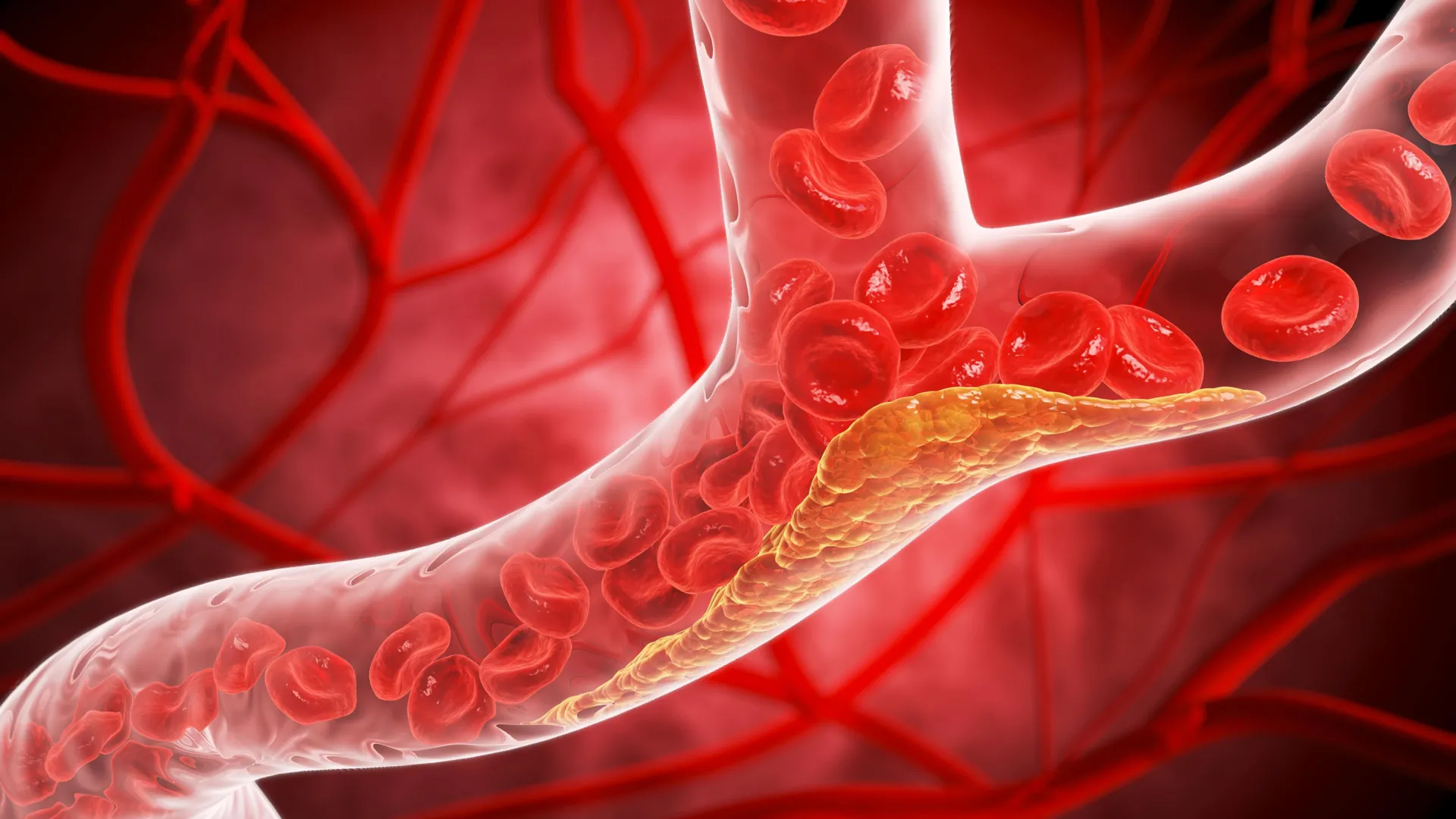
In the United States, approximately one in four adults currently grapples with elevated LDL-C. This condition is the primary driver of atherosclerosis, the process by which lipids accumulate within artery walls to form plaque. This plaque restricts vital blood flow and, if it ruptures, can trigger catastrophic cardiac events. Despite the availability of modern medicine, the prevalence of these conditions underscores the need for a more proactive clinical framework.
A Chronology of Clinical Evolution
The road to these 2026 guidelines has been marked by a decade of rapid innovation in cardiology. Since the 2018 guidelines, several major clinical trials have redefined our understanding of lipid-lowering therapies and the genetic components of heart disease.
- 2018: The previous landmark guidelines were established, emphasizing statin therapy and the use of non-statin medications for high-risk patients.
- 2019–2024: A period of intensive research followed, including the emergence of PCSK9 inhibitors and the refinement of coronary artery calcium (CAC) scoring as a predictive tool.
- 2025: Large-scale data analysis from the PREVENT risk model project neared completion, incorporating data from over 6.6 million patients.
- March 2026: The official unveiling at the ACC’s 75th Annual Scientific Session marks the formal adoption of these updated standards, transitioning cardiology into a new, data-driven era.
Supporting Data: The Power of the PREVENT Calculator
Perhaps the most significant technical upgrade in the 2026 guidelines is the introduction of the Predicting Risk of Cardiovascular Disease EVENTs (PREVENT) calculator.
For years, clinicians relied on models that assessed 10-year risk primarily in patients aged 40 and older, using a limited set of variables. The PREVENT model marks a paradigm shift. It is designed for use starting at age 30 and integrates a much broader array of data points, including kidney function and blood sugar levels. Because it is calibrated against a dataset of 6.6 million people—a staggering increase from the 26,000 used in the previous models—it provides a more accurate and representative risk profile for a diverse population.
Long-Term Prediction
The new calculator allows for both 10-year and 30-year risk projections. By extending the horizon of risk assessment, physicians can identify "silent" risks in younger patients, enabling them to suggest lifestyle modifications or early pharmacological intervention before irreversible arterial damage occurs.
Rethinking Risk: Genetic and Demographic Enhancers
The 2026 guidelines explicitly move away from a "one-size-fits-all" approach. Recognizing that biology is not destiny, the writing committee has expanded the definition of "risk enhancers."
Beyond Basic Factors
Clinicians are now encouraged to look at a patient’s comprehensive medical and personal history. Key considerations now include:
- Genetic Conditions: Patients with familial hypercholesterolemia should now be screened as early as age 9.
- Lp(a) Testing: A one-time test for Lipoprotein(a) is recommended. Elevated levels of this particle are strongly tied to inherited risk; levels of 125 nmol/L can raise heart disease risk by 40%, while levels of 250 nmol/L can double it.
- Life Events: Physicians must now account for gender-specific risk factors, such as early menopause, preeclampsia, or gestational diabetes.
- Chronic Inflammation: The use of high-sensitivity C-reactive protein (hsCRP) tests is now recommended to gauge underlying systemic inflammation, which can exacerbate plaque formation.
Official Responses and Clinical Philosophy
The guideline committee emphasizes that while medical technology has advanced, the foundations of health remain rooted in the basics. "Roughly 80% to 90% of cardiovascular disease is linked, at least in part, to factors people can modify," Dr. Blumenthal notes. The committee continues to advocate for a balanced diet, regular physical activity, tobacco cessation, adequate sleep, and weight management as the bedrock of cardiovascular prevention.
Dr. Seth Martin, a cardiologist and committee member, highlights the necessity of this shift: "Shifting the paradigm toward proactive prevention strategies earlier in life can meaningfully change the trajectory of cardiovascular disease and lead to better health outcomes for people decades later."
Implications for Clinical Practice and Treatment
The 2026 guidelines broaden the therapeutic toolkit available to clinicians. While statins remain the first line of defense, the guidance now provides clear pathways for utilizing:
- Ezetimibe: For further reduction in LDL.
- Bempedoic Acid: An effective option for those intolerant to statins.
- PCSK9 Inhibitors: Injectable monoclonal antibodies that offer potent cholesterol reduction for high-risk individuals.
New LDL-C Targets
The targets have become more aggressive to match the seriousness of the disease:
- Low-Risk Individuals: Optimal LDL-C should be below 100 mg/dL.
- Intermediate-Risk Individuals: Target levels below 70 mg/dL.
- High-Risk Individuals: Target levels below 55 mg/dL.
The inclusion of targets for non-HDL cholesterol and apolipoprotein B provides clinicians with additional metrics to ensure patients are not just hitting a "number" but are truly achieving a state of metabolic health that protects the arteries.
Looking Toward the Future
The 2026 guidelines are not static. The inclusion of an editorial discussing the findings of the VESALIUS-CV clinical trial suggests that the medical community is already looking toward even more aggressive management. Evidence from such trials indicates that for patients with established, moderate atherosclerosis, lowering LDL-C to below 55 mg/dL through combination therapy may be the future of standard care.
The development of these guidelines—a collaboration between the ACC, the AHA, and various cardiovascular health organizations—serves as a blueprint for the next decade of heart care. By integrating advanced risk calculation, early genetic screening, and personalized therapeutic targets, the 2026 guidelines provide a sophisticated roadmap for reducing the burden of heart disease. For patients, the message is clear: the sooner you understand your individual risk, the more effectively you can partner with your clinician to secure a healthier, longer life.